INTRODUCTION
Numerous surgical techniques to treat acute high-grade acromioclavicular (AC) joint dislocation have been reported in previous studies [1-5]. Opening fixation techniques, such as using a hook plate or Bosworth screw, are still widely used. Arthroscopic fixation techniques have recently been developed and used in a variety of ways to treat AC joint dislocation [6]. However, the optimal surgical treatment of these options is still unclear.
The stability of the AC joint is maintained mainly by the coracoclavicular (CC) and AC ligaments. The CC ligament is composed of conical and trapezoid ligaments, which play an important role as vertical stabilizers of the AC joint. Surgical treatment is recommended for Rockwood Type III and V injuries due to AC joint instability caused by a complete rupture of the CC and AC ligaments by higher energy trauma [7].
Hook plate fixation is a reliable and widely used treatment for AC joint dislocations. However, the role of the clavicle hook plate is to produce nonanatomical reduction of the AC joint, which may have negative effects on the shoulder rehabilitation process and can lead to loss of reduction following plate removal. In addition, this technique has the disadvantage of requiring a second operation to remove the plate. Arthroscopically, cortical button fixation has recently been introduced and has shown successful results, including several advantages over open procedures [8]. However, this arthroscopic fixation technique is concerning regarding its ability to provide horizontal stability; several complications related to metals have been reported, such as loss of CC reduction and risk of fracture of the clavicle or coracoid process [1,9].
Recently, Lee et al. [5] introduced an arthroscopic CC fixation technique that uses multiple soft anchor knots to overcome these complications and reported satisfactory clinical outcomes. Their technique ensured both horizontal and vertical stability to the AC joint while maintaining anatomic fixation [5]. Today, more than 150 surgical and conservative treatment options have been described to treat AC joint dislocations, although many are controversial. The present review summarizes the currently available data regarding surgical options for acute high-grade AC joint dislocation.
CLASSIFICATION
The most commonly used classification for AC joint dislocation is the Rockwood classification system [10]. This approach is based on radiological findings and classifies AC joint dislocations into six types. Low-energy trauma injuries, which are classified as type I or type II injuries, are treated conservatively using a Kenny-Howard brace [11]. In contrast, high-energy trauma injuries, such as type IV, type V, and type VI injuries, are treated surgically [12], while the treatment for type III injuries is still being debated [13].
SURGICAL PROCEDURES
Hook Plate Fixation
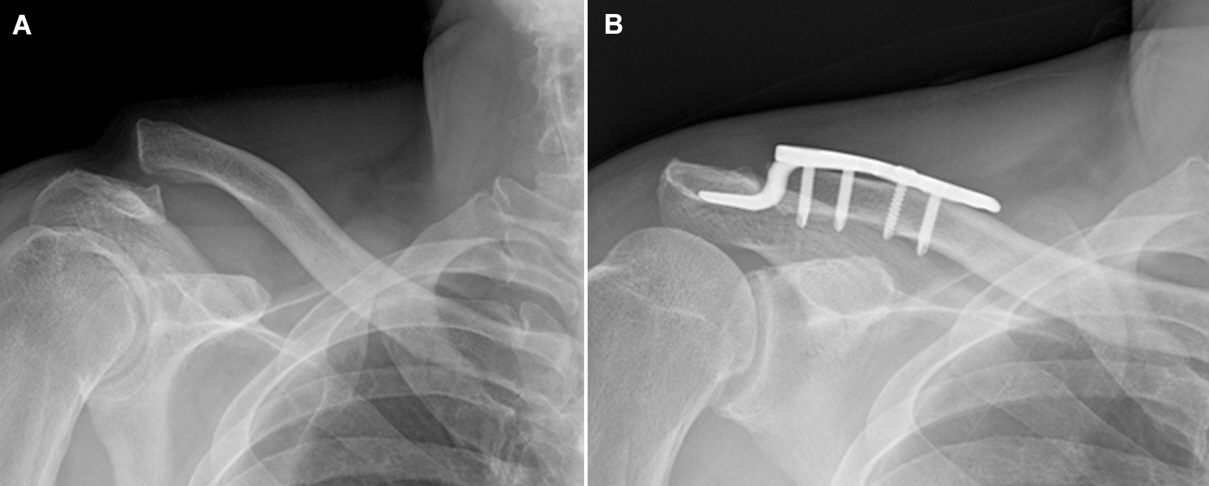
AC joint fixation allows time for the native AC and CC ligaments to heal in place by reducing the AC joint and maintaining the reduced AC joint. Hook plate fixation is one method of primary fixation across the AC joint (Fig. 1). In this fixation method, the hook portion of the plate is positioned beneath the acromion, and the plate is then fixed to the clavicle with screws to maintain adequate reduction of the AC joint. The technique can be used to treat acute injuries and may be combined with ligament reconstruction for chronic injuries with good short-term outcomes. Kienast et al. [14] used AC hook plate fixation to treat 225 patients with Rockwood type III–V AC joint dislocations and reported excellent or good outcomes in 89% of patients; however, the overall rate of complications was relatively high (10.6%). It is not rare for hook plate fixation to result in serious complications, including upward cutting of the hook through the acromion [15], subacromial osteolysis [16], fracture [17], AC joint osteoarthritis, subacromial impingement, and rotator cuff tears [18]. In vivo analyses of AC joint motion after hook plate fixation have indicated that clavicular motion and AC joint biomechanics change significantly after hook plate fixation [19]. The main disadvantage of this surgical procedure is the need for a second surgery to remove the implanted hardware.
Bosworth Screw Fixation
In 1941, Bosworth [20] introduced a fixation technique involving placement of a screw between the clavicle and the coracoid. Typically, a 6.5-mm partially threaded cancellous screw is used. Most surgeons favor open screw insertion, as percutaneous techniques are associated with a high rate of technical failure (32%) [21]. According to Rockwood et al. [22], five types of motion between the coracoid and the clavicle can lead to fatigue or failure of the implant over time. Because of the high rate of hardware migration and screw breakage over time, reoperation is usually required between 8 and 12 weeks after the initial surgical procedure [23].
Arthroscopic Fixation of the CC Joint
Arthroscopic-assisted procedures with CC suspension devices aim to increase the healing ability of torn AC and CC ligaments and reduce the CC distance. In the management of AC joint injuries, arthroscopy-assisted procedures provide several advantages over open procedures. These techniques offer superior visualization of the base of the coracoid and require less soft tissue dissection and smaller incisions than open procedures [24]. Additionally, arthroscopic techniques have the theoretical benefit of allowing the surgeon to identify and treat associated injuries within the glenohumeral joint and subacromial space [25].
The TightRope/EndoButton/Dog Bone technique
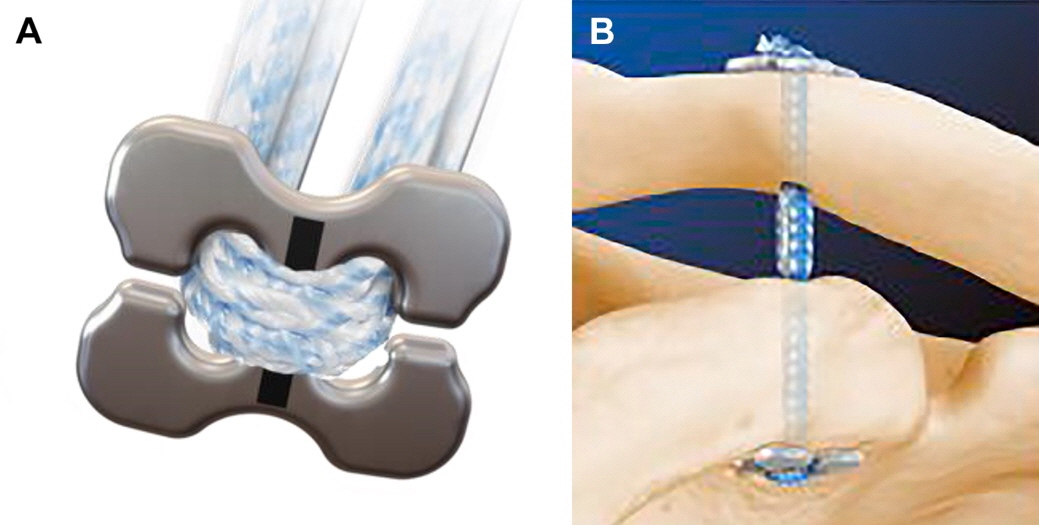
A prosthetic CC suspension device, such as the TightRope device (Arthrex, Naples, FL, USA), can also be implanted (Fig. 2). This device contains titanium buttons placed on top of the clavicle and under the coracoid that are connected with a continuous loop of no. 5 FiberWire suture (Arthrex). A similar device, the EndoButton device (Smith & Nephew, Memphis, TN, USA), was also used with a no. 5 Ethibond suture (Ethicon Inc., Somerville, NJ, USA) (Fig. 3). The TightRope device was based on the principles of the EndoButton system [26]. Subsequently, the Dog Bone device (Arthrex) (Fig. 4), which is similar to the TightRope/EndoButton devices, has also been introduced [27].
Using these single metallic suspension devices anchored at the isometric point of the CC ligament, good clinical results have been reported in many other studies; however, the risk of secondary subluxation is a concern [28]. The most commonly reported complication was hardware migration into the clavicle, coracoid, or both. The rate of migration was as high as 89% as reported by Scheibel et al. [29]. In addition, many patients complain of persistent symptoms after surgery related to hardware irritation over the superior clavicle fixation site [9].
Since vertical placement of these single metallic suspension devices does not replicate the normal orientation of the CC ligaments, this non-anatomic technique has recently been criticized in biomechanical studies [30]. Therefore, while vertical stability may be restored, horizontal instability may persist [31]. Theoretically, the use of two or more vertical stabilizers along the course of the CC ligament can better restore the anatomical and biomechanical properties of the natural ligaments [30]. Scheibel et al. [29] published good to excellent early clinical results using arthroscopic-assisted techniques with two TightRope devices in 28 patients with acute AC joint dislocation. In addition, Venjakob et al. [32] reported reliable stability of AC joints in 96% of patients in a study of arthroscopic-assisted, double EndoButton device procedures to treat AC joint dislocation with a mean follow-up duration of 58 months [32].
Despite these favorable results, the use of two metallic CC suspension devices risks fracture of the clavicle or coracoid process due to the non-negligible diameter of the drill holes, 4.0 mm [33-35]. Martetschläger et al. [36] showed that 20% of the fractures of the clavicle or coracoid process were related to complications resulting from technical errors in the drilling technique. Despite these technical surgical problems, the TightRope/EndoButton/Dog Bone techniques had the lowest rate of radiographic failure at only 5% of patients with recurrent dislocation.
Multiple all-suture anchor technique
CC suspension devices, such as the 1.8-mm Y-Knot Flex All-suture Anchor (ConMed Linvatec, Utica, NY, USA), were used. In contrast with procedures that use metal knots, soft knots are anchored at the bottom of the coracoid process at the entrance to the tunnel. The use of three vertical stabilizers rather than a single vertical stabilizer was intended to restore horizontal stability as well as vertical stability, as in the suspension bridge principle (Fig. 5). It is important to create small-width bone tunnels to reduce the risk of clavicle or coracoid process fractures [37]. Recently, Lee et al. [5] reported satisfactory clinical outcomes at a mean follow-up of two years in 27 patients with acute high-grade AC joint injury treated with an arthroscopic CC fixation technique using multiple soft anchor knots. These outcomes are likely due to the small tunnel width and multiple strands used, which allow for safe fixation while minimizing complications of metallic fixation and providing strong vertical and horizontal stability. It is important to note that the learning curve for this procedure is steep because it is technically demanding. Nevertheless, according to currently available biomechanical and clinical evidence, multiple all-suture anchor fixation can be considered a feasible and reliable treatment strategy for AC dislocation.
CONCLUSION
AC joint dislocation is a relatively common injury in the general population. A large proportion of these patients demonstrate acute high-grade AC joint injury that requires surgical treatment. Surgical treatment methods have made great progress in the past 30 years, and various surgical procedures are suitable for treatment of AC joint injuries. However, no gold standard procedure has been established. It is therefore vital to consider various surgical treatments depending on patient age and physical needs and the surgeon’s proficiency.