INTRODUCTION
Distal-third humeral fractures account for up to 2% of all adult fractures [1], and they are challenging to surgically correct [2-4].Various anatomical precontoured locking plates have recently been developed and are used for surgical treatment of distal humerus fractures [5-7]. Extra-articular distal humerus locking plates (EADHPs; DePuy Synthes, Oberdorf, Switzerland) are anatomical precontoured plates widely used in distal humeral extra-articular diaphyseal fractures [8-12].
The posterolateral elbow column is used to fix the EADHP with a posterior approach. Despite the distally tapered design of the plate, it causes plate protrusion and skin discomfort after surgery (Fig. 1). Implant prominence after EADHP fixation was noted in up to 59.5% of cases [13]. This problem requires implant removal after fracture union [11,12]. However, in most distal humeral fracture cases, EADHPs should be placed beneath the radial nerve (Fig. 2). Thus, iatrogenic radial nerve palsy is likely to result from EADHP removal surgery.
Zhou et al. [14] reported that EADHP caused approximately 8º of anatomic fit mismatch in the shafts of adult Chinese bodies in a cadaveric humeri study, which can be resolved by bending the plate. However, anatomic fit mismatch with plate protrusion occurring at the EADHP distal tip is likely to occur when the humerus is small, and anatomic fit mismatch is difficult to resolve through plate bending. Therefore, it is necessary to predict the plate protrusion occurrence and resulting skin discomfort that leads to risk of iatrogenic radial nerve palsy to better inform treatment planning and implant selection. However, the humeral size at which EADHP distal tip protrusion occurs due to anatomic fit mismatch has not been established.
The purpose of this study was to determine the humeral size cutoff for plate protrusion despite proper plate positioning through a cadaveric study. We hypothesized that the smaller the size of the humerus, the greater the anatomic fit mismatch of EADHP that would occur, and that the relationship between humeral size and mismatch will have a negative linear correlation.
METHODS
Because this study is a cadaveric study, there is no Institutional Review Board approval and informed consent for this study.
Specimens
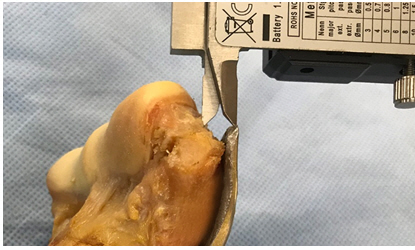
A total of 20 humeri of various sizes were used. All soft tissue was removed, and the lack of any gross deformities of the humerus was confirmed. Humeral length and distal humeral width were used as parameters of humeral size. Humeral length was measured along the anatomical axis, and the distance between the humeral head tip and the trochlear tip with a perpendicular line on the axis was measured using digital tape (BL-DM; Bluetec, Daejeon, Korea). Distal humeral width was measured as the medial-to-lateral length between the medial and lateral epicondyles along the perpendicular plane of the anatomical axis using a digital caliper (SD500-150PRO; Sincon, Busan, Korea) (Fig. 3).
Measurement of Anatomic Fit Mismatch
A six-hole EADHP was positioned sufficiently laterally to not encroach on the olecranon fossa. EADHP mismatch caused by humeral posterior angulation in the shaft area as well as in the distal part was due to the plate’s distal five holes being longer than that of the distal humeral posterolateral column. The shaft mismatch could be resolved through proper EADHP bending [14], so the middle portion of the EADHP was bent using a plate bending press (Plate Bending Press 329.3; DePuy Synthes) to fit the contour of posterior angulation of the humerus. Additionally, mismatch occurring at the plate distal tip may be improved by proximal plate positioning, but in such cases, plate-bone mismatches occurred at the posterolateral column even if the plate was modified by the plate bending press. Therefore, we first fitted the EADHP to the posterolateral column, the mismatch occurring in the humeral shaft was resolved by the plate bending press, and the mismatch occurring in the plate distal tip was measured. The amount of mismatch between the plate and distal humerus was assessed by measuring the distance between the center point of the EADHP distal tip and the distal humeral bone point. The distal humeral bone point was set as a perpendicular line drawn from the plate distal tip center point to the humeral bone (Fig. 4). There have been no previous studies of EADHP anatomic fit mismatch and symptom occurrence. We defined unacceptable EADHP anatomic fit mismatch as plate protrusion ≥10 mm.
Statistical Analysis
Simple linear regression was performed to estimate how humeral length and humoral width predicted protrusion distance. Receiver operating characteristic curve analysis was used to determine the appropriate cutoff value for plate protrusion, and the value with the largest Youden index (J) was defined as the optimal cutoff value [15]. Statistical power was set to 0.9 and the threshold for significance was set to p≥0.05. All statistical analyses and tests were performed using IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Mean humeral length was 301.13±23.3 mm and mean distal humeral width was 60.9±5.0 mm. Mean plate protrusion distance was 9.1±2.7 mm. In total, 45% (9/20) of humeri showed ≥10 mm plate protrusion. A significant linear correlation was observed between humeral length and plate protrusion (p=0.001) and the coefficient of determination value (R2) was 0.477. The best-fit linear equation was Y=32.85–0.08X (Fig. 5A). A significant linear correlation was also confirmed between distal humeral width and plate protrusion (p<0.001), and the R² was 0.814 and the best-fit linear equation was Y=38.57–0.48X (Fig. 5B).
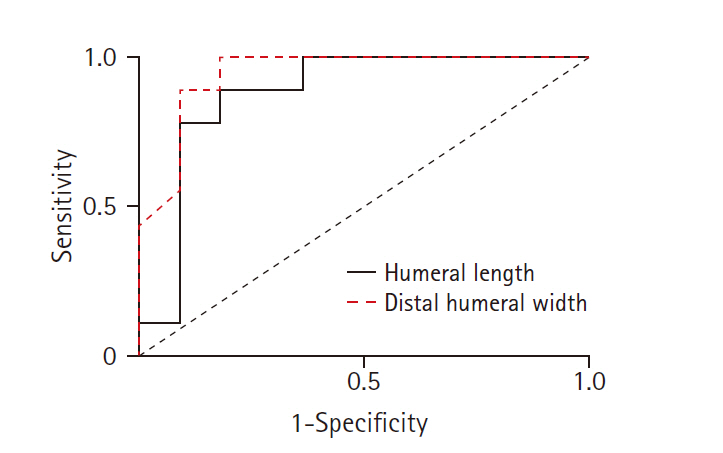
The area under the curve for humeral length was 0.879 and for distal humeral width was 0.944. The maximal J value for humeral length was 0.707; thus, the cutoff value for humeral length to avoid ≥10 mm plate protrusion was 293.6 mm (sensitivity, 88.9%; specificity, 81.8%). The maximal J value for distal humeral width was 0.818, and the cutoff value for humeral width was 60.5 mm (sensitivity, 100%; specificity, 81.8%) (Fig. 6).
DISCUSSION
The purpose of this study was to investigate whether anatomic fit mismatch between EADHP and the distal humerus increases as humeral size decreases when an EADHP is used to repair a distal humeral fracture. EADHP protrusion decreased by 0.08 mm per 1-mm increase in humeral length. As distal humeral width increased by 1 mm, plate protrusion decreased by 0.48 mm. Additionally, when humeral length was <293.6 mm or distal humeral width was <60.5 mm, plate protrusion was at least 10 mm at the distal humerus.
Despite the tapered design of the EADHP for the distal humerus, anatomic fit mismatch frequently occurred at the distal tip of the EADHP. The EADHP was designed to allow distal fixation with five locking screws (three bicortical screws proximally on the lateral column and two unicortical screws at the end toward the capitellum and trochlea) [11]. If EADHPs are proximally fixed to avoid distal tip protrusion in small-sized humeri, mismatch at the distal tip of the plate can be reduced to some degree, but a gap between the bone and plate occurs at the lateral column where the three bicortical screws are supposed to be fixed. If the gap is greater than 5mm, biomechanical stability is significantly decreased [16]. Therefore, these mismatches should be considered in preoperative planning.
Humeral length and distal humeral width were used as parameters for humeral size in this study. Distal humeral width was the most relevant measure, and it had approximately twice the R2 value of humerus length. In a previous cadaveric humeral estimation study, the R2 between the distance from the olecranon fossa upper margin to the trochlear tip and humeral length was 0.47 [17]. This R2 suggests that humeral length is not highly predictive of the size of the distal humeral region. Additionally, the R2 between humeral length and plate protrusion as measured in this study was 0.477, which was similar to previous values observed between the distal humerus region and humeral length. Interestingly, the R2 between distal humeral width and protrusion was 0.814, suggesting that distal humeral width is a better predictor of plate protrusion than humeral length.
Zhou et al. [14] reported a mismatch issue for EADHPs in the distal humerus posterolateral column and shaft in a Chinese cadaveric study. They found that 75% (33/44) of humeri were longer than 293.6 mm, which is the cutoff value for plate protrusion in this study. However, they focused on mismatch at the shaft, not at the distal tip of the EADHP. Furthermore, plate-bone mismatch due to angulation of the shaft area can be resolved through plate bending, but distal plate protrusion is difficult to resolve, so it is necessary to predict whether the patient is an EADHP candidate before surgery.
EADHP anatomic fit mismatch should be predicted preoperatively to prevent implant removal and potential iatrogenic radial nerve damage. Trikha et al. [13] reported that approximately 59.5% (22/37) of patients treated using an EADHP exhibited prominence on the elbow posterolateral side. Among them, only one patient underwent implant removal. Although implant mismatch occurred, not all patients developed skin discomfort requiring implant removal. However, in the majority of cases, the EADHP is placed beneath the radial nerve in a posterior approach to distal humeral fractures, and no matter how cautious we are, iatrogenic radial nerve palsy can occur during implant removal. Thus, when skin protrusion due to EADHP anatomic fit mismatch at the distal tip and resulting discomfort are expected, alternative treatments should be considered.
As an alternative treatment, a lower profile plate for the distal medial tibia can be employed for distal humerus fractures through the same posterior approach [18]. This locking plate does not use the posterolateral column of the distal humerus and seems to be less affected by protrusion; however, whether the biomechanical properties of the plate are comparable to conventional EADHPs should be investigated. As another alternative, a locking compression plate used for the proximal humerus was suggested via an anterolateral approach [19,20]. A previous biomechanical study showed that modified use of a proximal humeral locking plate has comparable mechanical stability compared to EADHP [21]. Yin et al. [22] suggested both an anterolateral approach and a lateral approach to distal humeral extra-articular fractures as alternative surgical methods. Unlike EADHP, plate irritation was not reported in the clinical outcomes of the anterolateral approach or the lateral approach.
There are several limitations to this study. First, cadaveric studies have some important differences from in vivo studies. In this cadaveric research, the soft tissue was completely removed, but soft tissue dissection is limited during in vivo surgery. Second, the definition or threshold value for EADHP anatomic fit mismatch leading to skin protrusion and related discomfort was determined arbitrarily, because research on this topic is sparse. The threshold leading to protrusion and discomfort in patients may not be consistent with this value. Third, the sample size was small.
In conclusion, anatomic fit mismatch in distal humeral fractures after EADHP fixation has a negative linear correlation with humeral length and distal humeral width. In particular, for patients whose distal humeral width is less than 60.5 mm, 10 mm or greater plate protrusion is predicted when an EADHP is applied, and an alternative implant or approach should be considered during treatment planning.