A Monteggia fracture is a fracture of the proximal ulna with proximal radioulnar ligamentous instability that leads to radial head dislocation [1-3]. In 1967, Bado [1] divided Monteggia fractures into four types based on direction of radial head dislocation and ulnar fracture angulation. A type I Bado fracture is a proximal ulnar anterior apex fracture with anterior dislocation of the radial head and is the most common type in children. A type II Bado fracture is a proximal ulnar anterior apex fracture with posterior dislocation of the radial head and is the most common type in adults. A type III Bado fracture is an ulnar metaphyseal fracture with lateral or anterolateral radial head dislocation, and a type IV Bado fracture is a fracture of both forearm bones that is accompanied by anterior dislocation of the radial head.
However, over the years, other injuries such as radial head fracture, coronoid fracture, or concomitant coronoid and radial head injuries have added complexities to the classification of Monteggia-related lesions [4]. As a result, the term Monteggia fracture includes various forms of complex fracture dislocations of the proximal ulna and radius; these have not yet been fully categorized. In this study, we report a rare variation of a Monteggia-like lesion and its management.
CASE REPORT
This study was approved by Institutional Review Board of Tehran University of Medical Sciences. Written consent for the study and publication of the photographs was obtained from the patient. The patient is a 24-year-old man who suffered from pain, swelling, and limited forearm and elbow movement following a motorcycle to car accident and who was referred to our trauma center emergency ward. Physical examination of the patient showed no symptoms of neurovascular disorders or of compartment syndrome. After initial supportive measures, radiographs of the elbow and forearm were obtained. Radiographs and computed tomography scan showed proximal and distal (segmental) fractures of the ulnar shaft, a proximal radial shaft fracture, and a comminuted radial head fracture (Fig. 1). Based on these results, the patient was deemed to be a candidate for surgery.
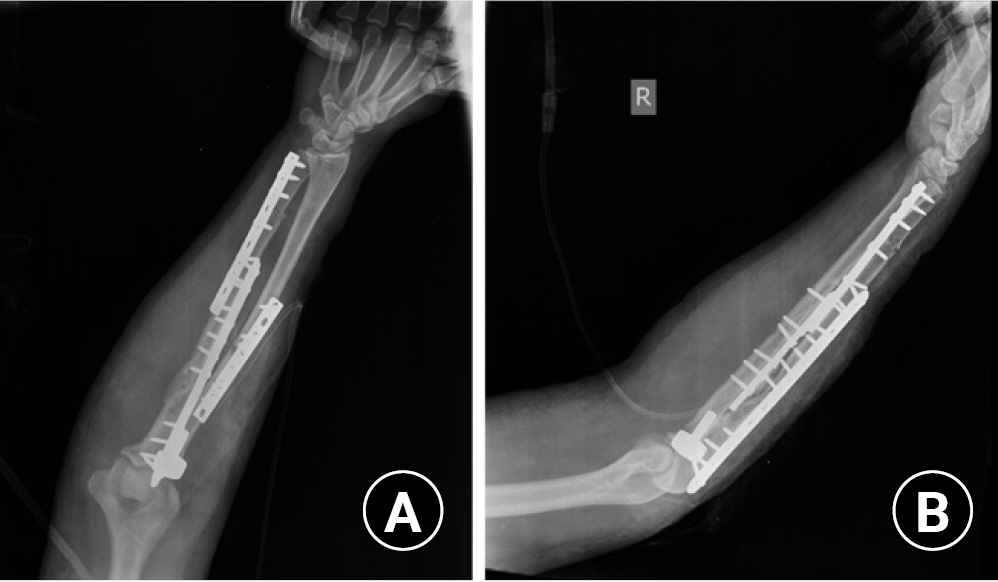
An inflated tourniquet was applied at the time of surgery. The ulna was exposed by a longitudinal incision from the olecranon to the distal ulna between the flexor carpi ulnaris and the extensor carpi ulnaris muscles. A 13-hole locking compression plate and a 10-hole dynamic compression plate were used in an overlapping fashion for ulnar fixation (Fig. 2).
The tourniquet was deflated, hemostatic measures were performed, and the subcutaneous and skin incisions were closed. The tourniquet was then inflated again, and the supinator muscle was located through the Thompson approach between the extensor carpi radialis brevis and extensor digitorum communis muscles. As the posterior interosseous nerve traversed through the supinator muscle, we identified and protected the posterior interosseous nerve from injury during surgery. The radial shaft was exposed, and the fracture was reduced and fixed with a 9-hole dynamic compression plate (Fig. 2). The radial head was accessed through the proximal part of the same Thomson incision via the trans-extensor digitorum communis interval.
After removing the comminuted fragments of the radial head and preparing the canal, a modular radial head prosthesis (Wright Medical, Memphis, Tennessee, USA) was implanted. Joint stability was assessed, and the incision was sutured. A long-arm splint was applied with the recommendation of night use for the first postoperative month. During the first week after surgery, physical therapy was begun and involved protected active motions. This therapy progressed to active assistive motions after one month.
DISCUSSION
In 1967, Bado divided Monteggia fractures into four types based on direction of radial head dislocation and ulnar fracture angulation [1]. Monteggia fractures are rare, accounting for only 2%ŌĆō5% of all proximal forearm fractures [5]. Monteggia-equivalent fractures, defined as Monteggia fractures with radial head fractures, are even rarer [6]. There have been few studies on Monteggia variants, and there is no precise and agreed upon definition of the term Monteggia variant or Monteggia-equivalent lesion [7]. There are several reports of Monteggia-equivalent fractures with no available classification system. Arora S et al suggested some Monteggia-equivalent lesions based on their literature review. A distal humeral fracture with a proximal third ulnar diaphyseal fracture and distal radial metaphyseal fracture with anterior dislocation of the radial head was presented as an example of a Bado type IV fracture [8].
In 2015, Laun et al. [9] reported 10 adult cases of proximal ulnar and radial head fractures treated with ulnar fracture plate fixation and radial head prosthesis. None of these patients had a concurrent radial shaft fracture. Jung et al. [10] and Calderazzi et al. [7] reported 27 and 12 patients, respectively, with ulnar and radial head fractures as Monteggia-like fractures. These patients were surgically managed with ulnar fracture plate fixation and radial head prosthesis. Jung et al. [10] reported that this type of fracture is prone to complications; they reported a total of 17 complications in 11 patients of a total of 27 cases after two years of follow-up. However, Calderazzi et al. [7] reported good results in Monteggia-like lesions if the injury pattern was recognized and each component of the injury was addressed.
In this study, we introduced a new variant of the Bado type IV Monteggia fracture that has not been reported previously in either adults or children. Preliminary results of the patient after four months of follow-up indicate an elbow range of motion from 15┬║ of extension to 140┬║ of flexion and near normal forearm rotation compared to the uninjured side (Fig. 3). The patient has a disabilities of the arm, shoulder and hand (DASH) score of 90 and no instability on elbow examinations. Bado type IV Monteggia lesions are extremely rare in adults; to the best of our knowledge, there has been no report of a Bado Type IV Monteggia fracture dislocation accompanied by a radial head fracture dislocation. In surgical management of this case, we noted that these co-fractures caused radioulnar interosseous membrane injury; therefore, radial head excision was not reasonable, and we used a radial head prosthesis for the patient. The results four months postoperatively are excellent. We suggest this rare type of fracture be classified as a Bado type IV Monteggia-equivalent fracture. Timely surgical management with plating and radial head prosthesis of such fractures in adults results in a good prognosis.