INTRODUCTION
Humeral component fixation in total shoulder arthroplasty (TSA) may be achieved with polymethyl methacrylate cemented fixation or cementless, press-fit fixation. Traditionally, cementation has been utilized to ensure stable component fixation that aims to prevent aseptic loosening [1]. While this has long been considered the gold standard, cementless fixation has gained popularity in contemporary practice. This may be attributed to the lower surgical costs, shorter operative time [2,3], and relative ease of removal in revision operations compared to cemented components that can increase the risk of complications involving the proximal humerus upon removal [4]. However, use of press-fit fixation may be accompanied by concerns of implant loosening in primary anatomic TSA (aTSA).
Previous case series have shown that stress shielding, metaphyseal bone resorption, and high rates of radiolucency have been associated with cementless stems [5-7]. This may be attributed to implant design leading to nonphysiologic load distribution and subsequent adaptations in addition to the use of implants designed for cement fixation. However, few studies have directly compared rates of loosening with cemented humeral components in aTSA. With the increasing popularity of uncemented humeral stems, understanding the effect on clinical outcomes of the humeral fixation technique employed is essential. While many studies have compared the use of cement in reverse shoulder arthroplasty, these findings may not translate to aTSA due to different biomechanics that alter the load on the humeral stems [8,9].
Existing studies that compare humeral component cementation in aTSA have primarily focused on perioperative outcomes [3] or fail to evaluate postoperative outcomes for a long-term follow-up period of greater than 5 years [2]. Our present study is one of the first to assess long-term postoperative radiographic, range of motion (ROM) and patient-reported outcomes (PRO) in patients receiving a cemented versus cementless humeral stem during aTSA. Based on previous studies [2,10], we hypothesized that cemented fixation of the humeral component provides superior postoperative outcomes.
METHODS
This research has been approved by the Institutional Review Board of Icahn School of Medicine at Mount Sinai (No. STUDY-17-00684-CR001). The patients and their families were informed that data from the research would be submitted for publication and gave their consent.
Study Population
This study retrospectively analyzed data from all patients who underwent primary aTSA by a single fellowship-trained shoulder and elbow orthopedic surgeon (ELF) between February 1990 and June 2019 with minimum 2 years of follow-up. Patients were excluded if fixation technique could not be determined or if the follow-up time was less than 2 years. An exception to the follow-up time requirement was made for patients who underwent revision surgery prior to the 2 year mark.
Operative Technique
All TSAs were performed using the same technique via a deltopectoral approach by a single orthopedic surgeon. A subscapularis peel or lesser tuberosity osteotomy was used to retract the subscapularis and was subsequently repaired at the end of the surgery. Fixation technique and glenoid component choice were determined intraoperatively by the surgeon. The choice of cementation over press-fit was made based on intraoperative bone quality. If the bone stock was deemed osteopenic or of low quality, humeral stem fixation with bone cement was utilized. A keeled glenoid component was used if glenoid morphology or size risked pegged perforation. Standard cementation technique was employed; the canal was brushed and cleaned with pulsating jet saline lavage and a cement restrictor was placed. The canal was then prepared with a thrombin and peroxide soaked sponge. Cement was placed in the canal and pressurized prior to implant placement.
Clinical Evaluation
The primary clinical outcomes included ROM and patient reported outcome questionnaire assessments. Data were collected pre- and postoperatively by the operating surgeon and their team. ROM evaluation included forward elevation (FE), external rotation (ER), and internal rotation (IR). IR was measured by comparing the vertebral level achieved upon active IR as described by Amroodi et al. [11] Patient reported outcomes were evaluated utilizing the American Shoulder and Elbow Surgeon (ASES) score, Simple Shoulder Test (SST) score, and visual analog scale (VAS) score for pain. Implant survival was also evaluated. In this study, failure was defined as the requirement for revision surgery. Additionally, we evaluated functional survival by using the minimal clinically important difference (MCID) in ASES score (+14) as reported by Simovitch et al. [12] and Werner et al. [13].
Radiological Assessment
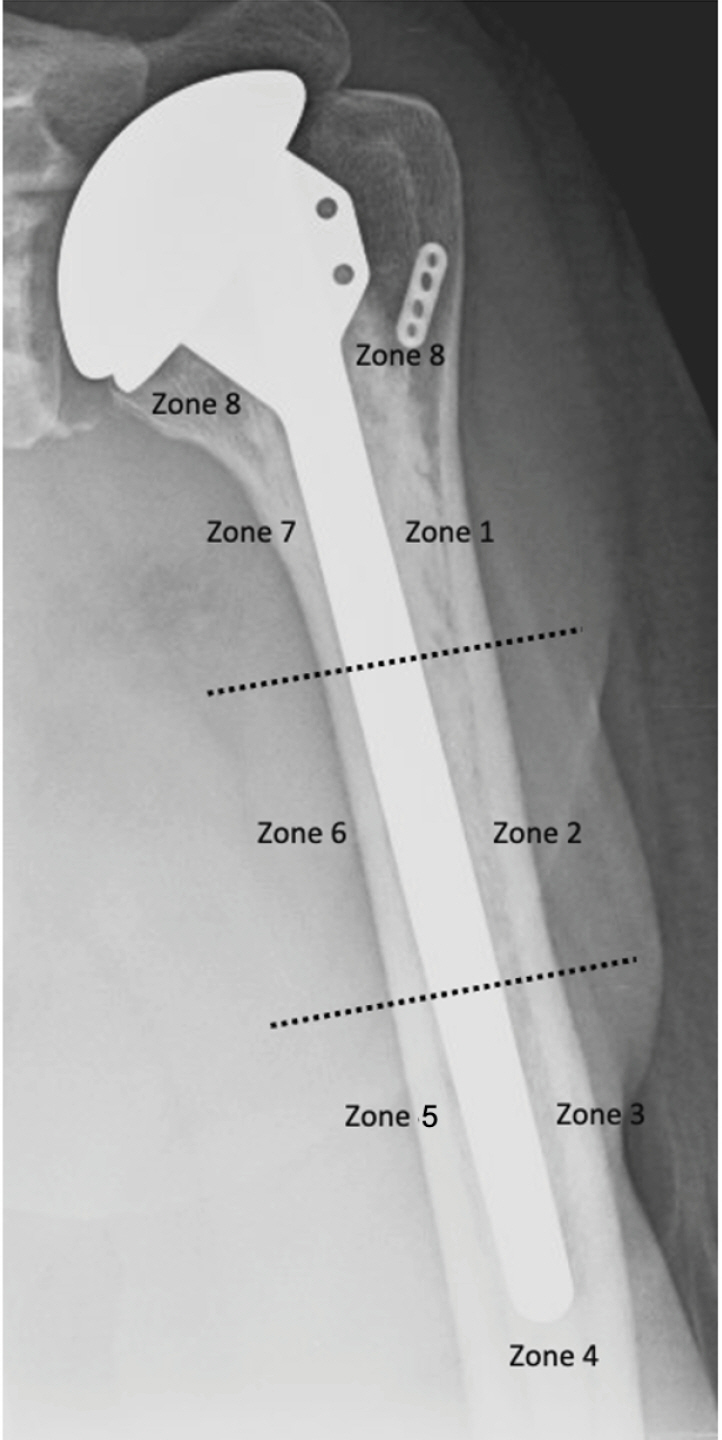
Postoperative radiographic analysis was performed independently by two fellowship-trained orthopedic surgeons (PJC, BOP). Analytic measurements utilized the immediate postoperative radiographs and radiographs collected at the most recent follow-up. The operating surgeon was limited in capacity to follow-up with all patients due to reduced clinical responsibilities. Radiographic measures assessed included the acromiohumeral interval (AHI) and humeral radiolucency. The AHI was defined as the distance (mm) between the humeral head articular cortex and the inferior acromion as described in Lehtinen et al. [14]. Correlation analysis was then conducted between AHI measurements and clinical outcome measures evaluated in this study. We evaluated correlations between both final AHI and the change in AHI. Finally, humeral radiolucency in humeral stems was defined as the presence of a radiolucent line in any of the eight radiographic zones measuring >2 mm at the cement-implant interface as described by Sanchez-Sotelo et al. [6,15] (Fig. 1).
Statistical Analysis
Analysis of all collected data was performed using Python version 3.8.8. Continuous variables were compared using a Student t-test, and categorical variables were compared using a chi-square test. For all statistical testing, a P-value <0.05 was considered significant. Kaplan-Meier survival curves were generated for implant survival (95% confidence interval), and 5-, 10-, and 15-year implant survival was assessed for both cemented and uncemented humeral implants.
RESULTS
Study Population
This study followed 134 patients (169 shoulders) who underwent aTSA. Included in final analysis were 138 cemented and 31 press-fit humeral stems. Three patients (three shoulders) were excluded due to the inability to identify fixation technique, and no patients were excluded for having a follow-up time of less than 2 years. The type of implant used within each cohort can be seen in Table 1. The mean age at time of surgery was 66.3┬▒8.6 years in the cement group and 55.6┬▒10.3 years in the press-fit group (P<0.001). The mean body mass index at the time of surgery was significantly higher in the press-fit group, 29.4┬▒3.8 kg/m2, than the cemented group, 26.6┬▒5.4 kg/m2 (P=0.016). No significant differences were seen between the two cohorts with regards to length of follow-up or sex. The mean follow-up length was 11.0┬▒5.7 years in the cement group and 9.4┬▒4.6 years in the press-fit group (P=0.147). In the cemented cohort the number of patients with <5, 5ŌĆō10, 10ŌĆō15, and >15 years of follow-up was 23, 45, 37, and 33, respectively. In the press-fit cohort the number of patients with less than 5, 5ŌĆō10, 10ŌĆō15, and >15 years of follow-up was 3, 15, 10, and 3, respectively. Of the 138 cemented aTSA procedures, 72 (52.2%) were performed on females, while ten of the 31 (32.3%) press-fit aTSA procedures were performed on females (P=0.071).
Clinical Outcomes
Within both the cemented and press-fit cohorts, significant and sustained improvements in ROM and patient reported outcomes were observed pre- to postoperatively. At the latest follow-up for all patients, no differences were seen in the ROM scores between the cemented and press-fit cohorts, FE (P=0.12), ER (P=0.60) and IR (P=0.77). However, patients who received a press-fit humeral stem reported better functional outcomes when compared to the cemented cohort. At final follow-up the mean VAS pain score was 2.2┬▒2.6 in the cemented cohort and 1.1┬▒1.9 in the press-fit cohort (P=0.038). ASES scores were significantly better in the press fit cohort, 86.5┬▒15.9 versus 73.6┬▒23.2 (P=0.005). Additionally, the SST scores were also significantly better within the press-fit cohort, 9.6┬▒3.2, when compared to the cemented cohort, 8.1┬▒3.3 (P=0.030). Pre- and postoperative values of all clinical outcomes are listed in Table 2.
Radiographic Outcomes
Radiographic analysis revealed that the AHI decreased significantly within both cohorts from immediately following surgery to final follow-up. The immediate AHI in the cemented cohort was 10.7┬▒4.1 and the final AHI was 8.3┬▒3.6 (P<0.001). The immediate AHI in the press-fit cohort was 14.3┬▒5.0 and the final AHI was 10.9┬▒4.6 (P=0.001). Humeral radiolucency was noted in two (1.5%) cemented implants and one (3.2%) press-fit implant. We identified no correlation between AHI (final and difference) and clinical outcome measures. Humeral radiolucencies were identified in both cohorts and evaluated as described by Sanchez-Sotelo et al. [6,15]. In the cemented cohort, radiolucency was identified in zone 8 of one implant and in zones 2 and 6 in the other. In the press-fit cohort, radiolucency was identified in zone 8. More details are indicated in Table 3 and Fig. 1.
Implant Survival
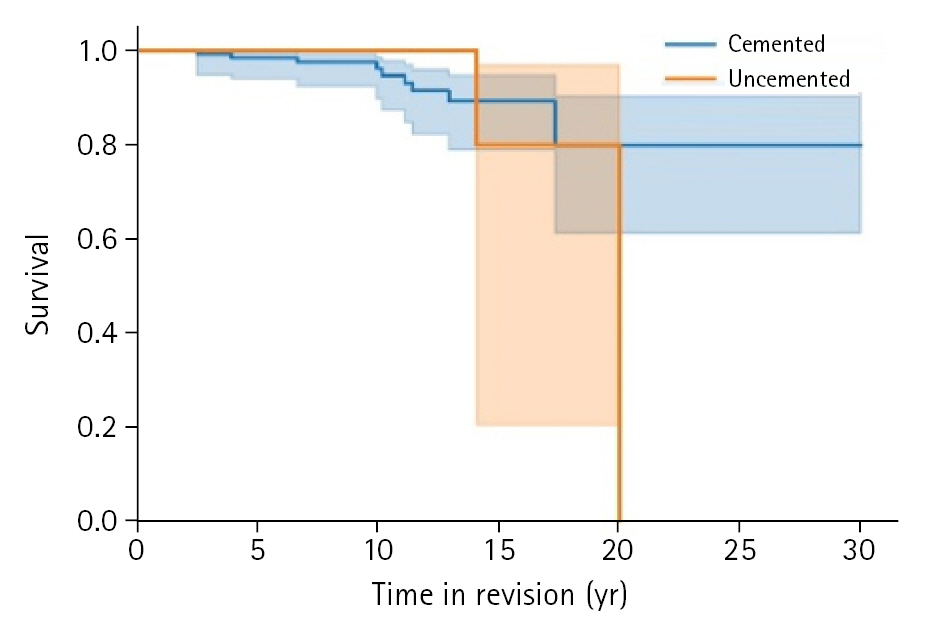
Both cemented and press-fit cohorts experienced excellent implant longevity with no difference in survival between cohorts (P=0.75) (Fig. 2). For the cemented cohort, 5-, 10-, and 15-year survival estimates based on the Kaplan-Meier (KM) analysis were 98.5%, 96.1%, and 89.3%. The press-fit cohort was similar with 100%, 100%, and 80% estimated survival rates. At the implant survival extremes, 12 cemented implants survived >20 years, but only one press-fit implant survived that long. In total, 12 revision surgeries performed, ten of the 12 were arthroscopic glenoid component removals with only two revisions necessary due to humeral loosening. One case of humeral loosening was reported in each of the cemented and press-fit cohorts (P=0.334). More details are indicated in Table 4. In addition to utilizing implant revision as an endpoint for measuring implant survival, we evaluated improvement sustainment through last follow-up. Utilizing an MCID of 14 ASES points as minimally acceptable, 12 shoulders in the cemented cohort and one shoulder in the press-fit cohort were deemed clinical failures (P=0.302).
DISCUSSION
While studies have evaluated the differences between cemented and press-fit humeral stems at short-term (>2 years of follow-up) and mid-term time points (>5 years of follow-up) [2,16], this is one of the first studies to report on long-term patient reported outcomes comparing cemented and press-fit humeral stems. In our study, we found that both cemented and press-fit humeral stems provide sustained and significant improvements in terms of shoulder function and pain. Both fixation techniques provide robust clinical outcomes following aTSA. At average follow-ups of 11 and 9.4 years, respectively, both cemented and press-fit patients demonstrated significant improvement in all ROM measurements with no significant differences between the two cohorts. This is in line with a previous meta-analysis comparing the two methods of fixation, which found that 80% of cemented studies and 82% of uncemented studies reported greater ROM postoperatively [16]. In their randomized control trial (RCT), Litchfield et al. [2] also found comparable ROM and PRO improvement between the two procedures.
Similar to ROM, we found significant improvements in all PROs with both fixation techniques. However, at final follow-up, VAS, ASES, and SST scores were significantly better in the press-fit group. Higher self-reported pain on the VAS in the cemented group may be due to increased patient susceptibility to pain due to increased age [17]. We also believe that differences in follow-up ASES and SST scores may be attributed to discrepancies in baseline values between the cohorts as press-fit patients also had higher scores preoperatively. A previous multicenter series of 64 short-stem, press-fit humeral components found similar improvements in VAS and ASES scores [18]. Our findings also correspond with Litchfield et al.ŌĆÖs RCT [2]. This group reported improved ASES scores with both procedures, but found no significant differences between the cohorts [2]. Their report was only at 1-year follow-up, and our results further demonstrate that both cemented and press-fit humeral stems significantly improve clinical ROM and PROs at long-term follow-up.
Regarding radiographic analysis, there was a significant decrease in AHI for both cohorts, with cemented stems having a narrower interval both immediately following surgery and at follow-up. Given the longevity of our follow-up and consistent with other studies, we expected to observe a decline in AHI over time [19]. However, neither cohort had a decrease in AHI below 6 mm, which is considered to be indicative of rotator cuff pathology [14,20,21]. Therefore, our results illustrate that the long-term integrity of the rotator cuff is effectively maintained in aTSA regardless of humeral fixation technique.
Another primary concern with the use of press-fit humeral stems is the advent of radiographic humeral radiolucency and aseptic implant loosening [6,7]. This is believed to be due to stress shielding and resultant bone resorption compared to cemented stems, which have a more homogeneous stress distribution [5]. Humeral radiolucencies cause concern in uncemented aTSAs as these have been correlated with worse ROM, functional outcomes, complication rates, and a higher risk of revision [22]. Furthermore, humeral components may be considered radiographically at risk for clinical loosening if there is a radiolucent line of 2 mm or greater in width present in three or more zones [6]. However, humeral radiolucency was only detected in two cemented and one press-fit stem over the course of our long-term follow-up, indicating that both provide functional radiographic outcomes with low risk of loosening. In line with our low rates of radiolucency, our study also found long-term survival of both cohorts at 5, 10, and 15 years. However, we should acknowledge the steep press-fit cohort drop off in the KM curve (Fig. 2). We have multiple cemented humeral stems operative even after >20 years, but only one press-fit implant survived as long. This one ultimately required revision. We hypothesize that within our study, this may be due to the later adoption of press-fit fixation as compared to cemented fixation.
As patients continue to live longer and healthier lives, implant survivorship and long-term efficacy are becoming increasingly important. A large institutional study conducted by Singh et al. reported 5-, 10-, and 20-year revision free survival rates of 94.2%, 90.2%, and 81.4% [10]. Within their analysis, press-fit stems had inferior survival rates when compared to cemented stems. However, in our study, both cemented and press-fit techniques yielded excellent survival rates at 5 years (98.5% and 100%, respectively), 10 years (96.1 and 100%, respectively), and 15 years (89.3% and 80%, respectively). Of note, the vast majority of failures were attributed to glenoid loosening. To the best of our knowledge, there are no studies on the association of humeral fixation technique with glenoid loosening. Only two revisions in our entire cohort were due to humeral loosening. One revision case due to the humeral component was reported in each cohort; however, we detected no significant difference in revision rates between groups. Additionally, compared to other studies evaluating clinical outcomes using similar MCID criteria, our patients fared similarly compared to a previously reported rate of 7.2% at 50 months [12]. Only 12 (8.7%) shoulders in the cemented cohort and one (3.2%) shoulder in the press-fit cohort failed to meet the MCID of 14 ASES points at a mean follow-up of 10 years. In all, both humeral fixation techniques experience low failure rates and deliver sustained and significant improvements in shoulder function.
We must address the limitations of this study. First, the relatively small number of failure events and unequal sample sizes make absolute comparisons across cohorts difficult. Additionally, we must acknowledge that a multitude of patient factors have been shown to affect outcomes following aTSA and that differences in cohort demographics, such as age and body mass index, could be confounders. The retrospective nature of this study coupled with long follow-up times resulted in multiple patients being lost to follow-up, dying, or seeking care at different institutions. As the patients included in this study spanned multiple decades, there have been numerous advances in implant technology and medical knowledge that may have influenced outcomes as well. One particularly significant advance is that the approval of reverse TSA in the early 2000s changed the management of shoulder pathologies with respect to the utilization of aTSA. Additionally, the preoperative and perioperative planning of procedures has improved significantly due to advances in medical imaging and three-dimensional modeling.
CONCLUSIONS
This long-term study followed a cohort of patients undergoing aTSA. In this series, we found that irrespective of humeral fixation technique, aTSA significantly improves shoulder function even after >10 years. However, within this cohort, press-fit stems provided comparable or better outcomes when compared to cemented stems with regard to patient-reported outcome scores.