INTRODUCTION
Total shoulder arthroplasty (TSA) is an effective surgical treatment for end stage glenohumeral arthritis not resolved by conservative treatment [1,2]. Anatomic TSA prostheses designs continue to evolve and there is a growing trend towards the use of bone-preserving prostheses as alternatives to traditional stemmed humeral implants [3-6]. Bone preserving prosthesis, such as Stemless TSA and humeral head resurfacing designs, are being compared to traditional stemmed TSA prosthesis [3,6-13]. Potential disadvantages include dependence on proximal bone stock [6]. TSA with a nonspherical humeral head and an inlay glenoid is one of the available bone-preserving prosthesis options. This implant aims to replicate the native anatomy of both the humerus and glenoid with the goal of restoring natural movement and improving component stability [14,15]. Numerous studies have reported excellent patient clinical outcomes with use of this prosthesis, but none of these prior studies reported outpatient complications [14-19].
Progressive improvements in shoulder arthroplasty techniques, perioperative protocols, and pain management strategies have allowed for increased utilization of outpatient TSA [20]. In addition, changes in healthcare policy with an increased focus on value-based medical care have further contributed to the rapid growth of outpatient arthroplasty [21]. Previous studies have described the success and safety of outpatient shoulder arthroplasty following the use of traditional stemmed TSA prostheses [1,17,20-23]. Despite the literature describing outcomes and complications following the use of traditional prostheses, few studies have evaluated complications and readmissions in the outpatient setting following the use of newer generation implants. Although outpatient arthroplasty rates are increasing, no large cohort studies describing 90-day complication rates for outpatient stemless TSA or humeral head resurfacing are available [6,24,25].
There is a paucity of literature describing complications of TSA and the safety of outpatient versus inpatient TSA surgery with a nonspherical humeral head and an inlay glenoid. The purpose of this study was to assess the 90-day complication profile of TSA with the above-mentioned prosthesis and compare early complication and readmission rates between patients undergoing inpatient or outpatient procedures. We hypothesized that TSA with a nonspherical humeral head and inlay glenoid could be performed safely in both the inpatient and outpatient settings with a low rate of early complications. Furthermore, we hypothesized that there would be no difference in complication or readmission rates between patients who underwent inpatient versus outpatient TSA.
METHODS
Patient Selection
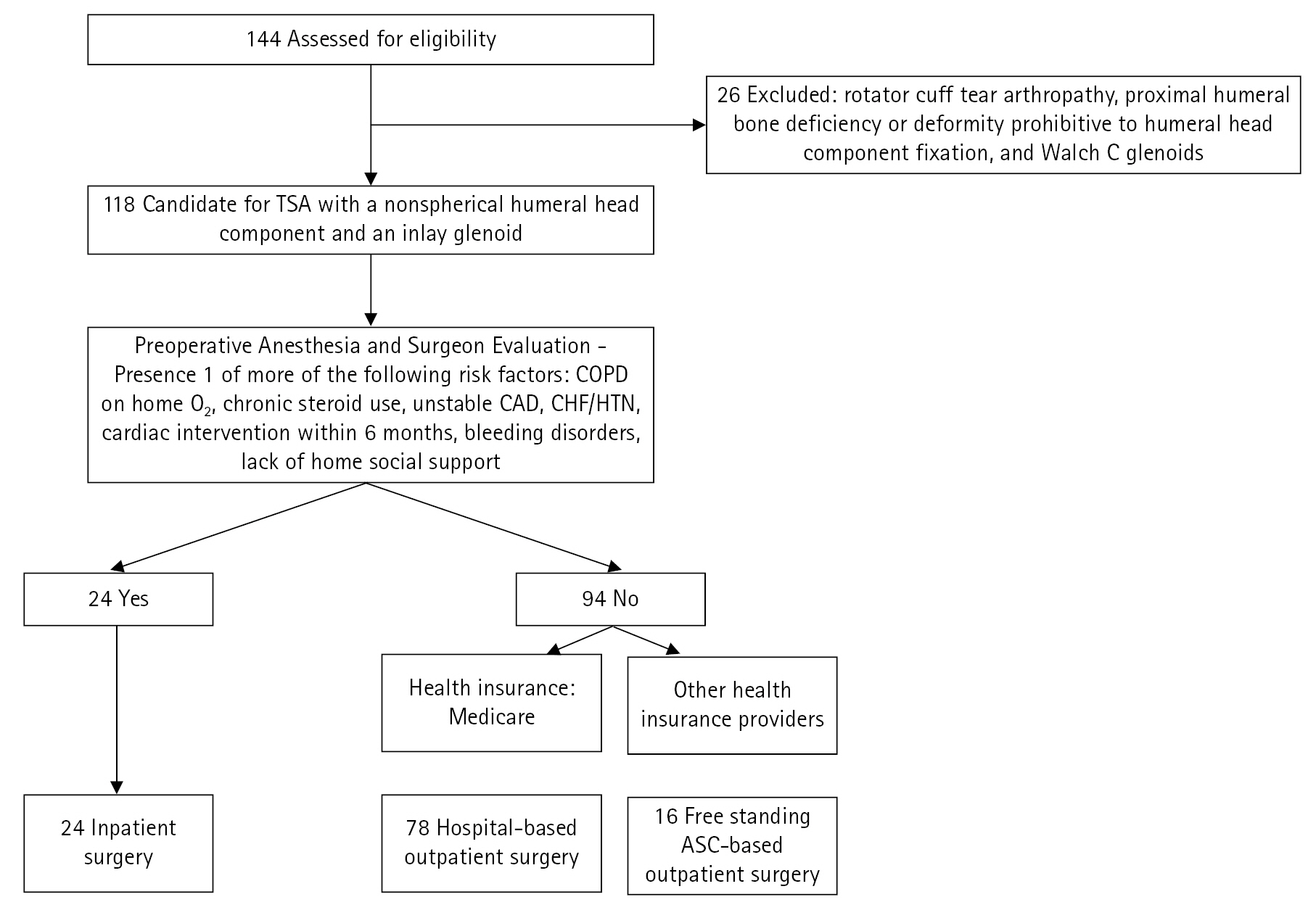
Institutional Review Board approval was obtained for the study (No. 5248). Informed patient consent was waived for this retrospective review by our Institutional Review Board. A retrospective chart review was conducted in a consecutive cohort of patients who underwent TSA with a nonspherical humeral head implant and an inlay glenoid replacement (Hemi-CAP OVO/Inlay Glenoid Total Shoulder System; Arthrosurface). Procedures were performed by a single surgeon (JPZ) between November 2017 and June 2022. Patient selection for this TSA prosthesis and the determination of surgical setting are outlined in Fig. 1. Inclusion criteria were primary glenohumeral osteoarthritis refractory to conservative treatment with an intact rotator cuff. Patients with Walch type A1, A2, B1, B2, and B3 glenoids, as diagnosed on preoperative axillary radiographs, were included [26]. Axillary radiographs have been shown to be comparable to computed tomography scans for glenoid staging [27]. Use of TSA with a nonspherical humeral head component and an inlay glenoid in Walch type A1, A2, B1, B2, and B3 glenoids is supported by multiple studie [3,16,18,19]. Exclusion criteria included diagnoses other than primary glenohumeral osteoarthritis, rotator cuff tear arthropathy, proximal humeral bone deficiency or deformity prohibitive to humeral head component fixation, and Walch C glenoids. Active smokers are not candidates for shoulder arthroplasty in the surgeon’s practice due to literature documenting increased complication rates [28,29].
Selection Criteria for Inpatient vs. Outpatient Procedures
TSA was performing in one of three surgical settings: inpatient surgery, hospital-based outpatient surgery, or outpatient surgery at a free-standing ambulatory surgery center (ASC). For inpatient procedures, the arthroplasty was performed at a hospital and the patient spent a minimum of 1 night in the hospital. For hospital-based outpatient procedures, the arthroplasty was performed at a hospital; however the patient was discharged home on the same day without spending the night in the hospital. For ASC-based outpatient procedures, the arthroplasty was performed at a free-standing surgical center, which is a facility physically independent of a hospital without an inpatient unit. Following TSA, the patient was discharged home directly from the post-anesthesia care unit at the ASC.
Patient selection for inpatient, hospital-based outpatient surgery, or ASC outpatient surgery was initially determined by preoperative anesthesia and surgeon evaluation (Fig. 1). A patient’s medical status was first assessed. Patients with the presence of one or more of the following medical or social comorbidities were selected for inpatient surgery: chronic obstructive pulmonary disease on home oxygen therapy, chronic steroid use, unstable coronary artery disease/congestive heart failure/hypertension, cardiac intervention within 6 months, bleeding disorders, and lack of home social support. Currently available risk prediction tools that aid in identifying patients who are appropriate for outpatient TSA [30-32] were not available for use when this study was initiated. Patients without the above medical or social factors were selected for outpatient surgery. The setting of their outpatient procedure, either hospital-based outpatient surgery or outpatient surgery at an ASC, was determined by their health insurance status. The Centers for Medicare and Medicaid Services (CMS) restricts coverage for TSA at ASCs; thus, all patients with healthcare coverage provided by CMS who were candidates for outpatient surgery underwent hospital-based outpatient procedures. Patients with other health insurance providers who were candidates for outpatient surgery underwent surgery at the ASC.
Surgical Technique
All TSA procedures utilized a nonspherical humeral head and an all-polyethylene inlay glenoid component. Patients received regional anesthesia with or with general anesthesia, as determined by anesthesiologist recommendations, and were placed in the beach-chair position. A standard deltopectoral approach with subscapularis tenotomy and biceps tenodesis was performed. Sizing guides were used to determine the true superoinferior (SI) and anteroposterior (AP) dimensions of the humeral head. For the ovoid humeral head component, the SI dimension was 4 mm larger than the AP dimension, with varying radiuses of curvature. After sizing, a guide pin was placed matching the patient’s native version and inclination. The humeral head was reamed to match the spherical undersurface of the component. Bony debris were removed and a tapered post was inserted into the humerus.
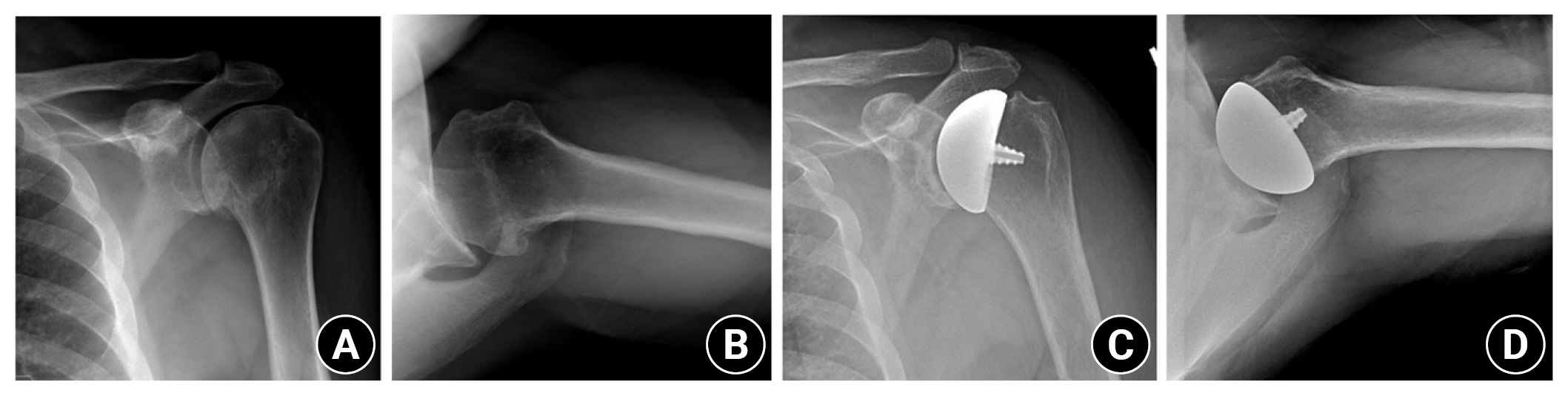
The glenoid was exposed and the reamer guide pin was placed on the center point on the glenoid. The glenoid was reamed, ensuring that the glenoid trial sat flush with the surrounding native glenoid surface. The glenoid component was inserted using a third-generation cement technique. After glenoid implantation, the definitive ovoid humeral head component was impacted over the post, engaging the morse taper. The subscapularis was repaired in all cases and standard closure was performed. Preoperative and postoperative anterior-posterior and axillary radiographs are presented in Fig. 2.
Postoperatively, patients’ arms were placed into a sling and they were immediately allowed pendulum exercises and range of motion of the elbow, wrist, and hand. At 2 weeks postoperatively, shoulder wall walks were allowed and formal physical therapy with a rotator cuff strengthening program was initiated. External rotation was limited for 6 weeks to protect the subscapularis repair.
Data Collection
Baseline patient characteristics and 90-day postoperative complications were collected from electronic medical records. A 90-day postoperative period was chosen to assess complications, readmission, and reoperations because this encompasses the global surgical period and appropriately reflects the medical postoperative course. Patient characteristics were age, sex, smoking status, body mass index (BMI), Charlson Comorbidity Index (CCI) score, American Society of Anesthesiologists (ASA) score, and location of surgery: either inpatient, hospital-based outpatient, or free-standing ASC.
Complications assessed within 90 days included medical and surgical complications as well as readmission. Medical and surgical complications included all adverse events as defined by the American College of Surgeons National Surgical Quality Improvement Program (ASC-NSQIP) [33], in addition to shoulder-specific complications. “Serious” adverse events were defined by ASC-NSQIP as follows: death, coma >24 hours, on ventilator >48 hours, unplanned intubation, stroke/cerebrovascular accident, thromboembolic event including deep venous thrombosis (DVT) or pulmonary embolism (PE), infectious complications (superficial surgical site infection, deep surgical site infection, organ/space infection, or sepsis), cardiac arrest, myocardial infarction, acute renal failure, return to the operating room, graft/prosthesis/flap failure, or peripheral nerve injury. “Minor” adverse events as defined by the ASC-NSQIP were wound dehiscence, blood transfusion, urinary tract infection, pneumonia, or progressive renal insufficiency. In addition, complications specific to shoulder arthroplasty were also assessed and included dislocations, wound complications, infections, subscapularis failures, tenodesis failure, hardware failure, periprosthetic fractures, arthrofibrosis, hematomas, and all-cause reoperations.
Statistical Analyses
All analyses were conducted with use of JMP software ver. 12 (SAS Institute). Means, standard deviations, and ranges are reported for continuous variables while frequencies and percentages are reported for categorical variables. The significance of differences in descriptive statistics between patient groups was evaluated with two-tailed t-tests and Fisher’s exact tests as statistically appropriate. P-values <0.05 were considered to be statistically significant.
RESULTS
Patient Demographics
One hundred eighteen TSAs in 111 patients were identified. Patient demographics, BMI, ASA score, CCI score, and surgical setting are presented in Table 1. Twenty-four patients (20%) underwent inpatient procedures while 94 patients (80%) underwent outpatient procedures. Among outpatient procedures, 78 of 94 (83%) and 16 of 94 (17%) were performed in the hospital-based outpatient and free-standing ASC settings, respectively.
90-Day Complications: All Patients
Complications are presented in Table 2. Within the 90-day postoperative period, four complications (3.4%) were observed: axillary nerve stretch injury, isolated ipsilateral arm DVT, ipsilateral arm DVT with PE, and upper gastrointestinal bleed (UGIB) requiring blood transfusion. Two patients (1.7%) required readmission. There were no dislocations, wound complications, infections, subscapularis failures, tenodesis failure, hardware failures, periprosthetic fractures, arthrofibrosis, hematomas, or reoperations.
One patient who underwent outpatient surgery was diagnosed with an axillary nerve injury postoperatively. The injury was attributed to intraoperative stretch neuropraxia and monitored with serial electromyography. At 9 months postoperatively, the nerve injury had completely resolved clinically and on electromyography following observational outpatient management. One patient who underwent outpatient surgery developed a DVT on their operative extremity, diagnosed on postoperative day (POD) 18, leading to a PE. This patient required readmission and was successfully treated with oral anticoagulation. Another patient who underwent outpatient surgery also developed a DVT on their operative extremity, diagnosed on POD 9, which was successfully treated on an outpatient basis with oral anticoagulation. One patient who underwent inpatient surgery developed a UGIB on POD 4, requiring readmission for a blood transfusion. She had a history of gastroesophageal reflux disease and clopidogrel use for coronary artery disease which was restarted postoperatively; however, she denied use of nonsteroidal anti-inflammatory drugs (NSAIDs). The patient was successfully managed medically.
90-Day Complications: Outpatient vs. Inpatient Surgery
Ninety-four patients (80%) had outpatient procedures, while 24 patients (20%) underwent inpatient procedures (Table 3). Patients who underwent outpatient procedures were significantly younger than those who underwent inpatient procedures (64.1 vs. 67.8, P=0.049). Furthermore, patients who underwent outpatient procedures had significantly lower ASA (2.4 vs. 2.8, P<0.001) and CCI scores (2.8 vs. 4.1, P<0.001) than those who underwent inpatient procedures. Between groups, there were no significant differences in the percentage females or BMI. There were also no significant differences om rates of 90-day complications (3/94 vs. 1/24, P=1.00) or readmissions (1/94 vs. 1/24, P=0.37) between the two groups. In addition, there were no significant differences between rates of any complication subtype between groups.
DISCUSSION
Our findings suggest that TSA with a nonspherical humeral head component and an inlay glenoid is associated with favorable short-term complication and readmission rates of 3.4% and 1.7%, respectively. Inpatient and outpatient TSA procedures were performed safely with no differences in complication rates or readmissions between surgical settings.
Shoulder arthroplasty is the primary treatment for patients with advanced glenohumeral osteoarthritis for whom conservative treatment has failed. Despite its growing use clinically, studies evaluating TSA, reverse total shoulder arthroplasty (RTSA), and hemiarthroplasty (HA) have reported concerning rates of readmissions and early medical and surgical postoperative complications [34-40]. At 90-days postoperatively, rates of complications range have been reported to range from 2.3% to 11% [35,36,41] and those of readmission from 1.8% to 11.2% [36,38,39]. Stemless TSA may be the most similar implant to TSA with a nonspherical humeral head and inlay glenoid, and while no large-cohort data 90-day studies exist, meta-analyses have reported that the short and mid-term complication rates following stemless TSA range from 8.3% to 9.7% [6,24,25]. In most reports, complications within 90 days were more likely to be medical than surgical, with the most frequent complications being related to the respiratory, renal, and cardiac systems, respectively [34,36,39]. Our 90-day complication rate of 3.4% and readmission rate of 1.7% are at the lower end of the ranges reported following the use of TSA, RTSA, HA, and stemless TSA. This comparison suggests that TSA with a humeral head component and inlay glenoid is safe and has a short-term complication profile similar to that of other TSA prostheses designs. In addition, similar to what has been reported in the literature, roughly 75% of our 90-day complications were medical in nature (DVT/PE and UGIB) while only 25% were surgical (axillary nerve stretch injury). There were no dislocations, wound complications, infections, subscapularis failures, tenodesis failures, hardware failures, periprosthetic fractures, arthrofibrosis, hematomas, or reoperations in our study.
Historically, use of bone-preserving humeral prostheses with improved glenoid stability has been prescribed for young active males who have higher rates of component loosening [4,10,35,42,43]. Advantages of bone-preserving shoulder arthroplasty prostheses include shorter operative and anesthesia time, a lower risk of periprosthetic fracture, less intraoperative blood loss, and easier revision options than traditional stemmed TSA prostheses [3,6-10,13]. Together, this may translate into fewer postoperative adverse events [11]. TSA with nonspherical humeral head and an inlay glenoid prosthesis aims to replicate the native anatomy, restore natural movement, and improve component stability [14,15]. Multiple studies have reported excellent patient clinical outcomes with use of TSA with this prosthesis design; however, no prior study evaluated outpatient complications [3,16,18,19].
In our study, there were no significant differences in either 90-day complication (3/94 vs. 1/24, P=1.00) or readmission (1/94 vs. 1/24, P=0.37) rates between patients undergoing outpatient or inpatient TSA. Outpatient shoulder arthroplasty is increasing in frequency and multiple studies that evaluated patients who underwent TSA, RTSA, or HA reported no significant differences in early postoperative complications between outpatient and inpatient cohorts [17,21,22,37,44]. Brolin et al. [44] and Bean at al. [45] reported that TSA and RTSA can be safely performed in a freestanding ASC setting; however no such research for TSA with a humeral head component and inlay glenoid exists. There were not enough ASC patients in our study to adequately power a comparison between patients who underwent outpatient hospital-based and outpatient ASC-based procedures. The lower proportion of procedures performed in the ASC setting may be due to TSA not being approved for CMS coverage at the time of this study.
In our study, outpatient TSA patients were significantly younger and had significantly lower ASA and CCI scores than inpatient TSA patients. These same demographic differences between cohorts have also been reported in the TSA, RTSA, and HA literature [37,44]. Patient selection is paramount for successful and safe outpatient shoulder arthroplasty; complications, and readmission rates all increase with patient age, female sex, and medical comorbidities [21,34,46]. Identifying higher-risk patients preoperatively is essential, as they may be more appropriate candidates for inpatient procedures. Multiple risk prediction tools have been developed to aid in identifying patients appropriate for outpatient TSA [30-32]. These tools can improve patient selection for same day discharge while minimizing perioperative complications. Eventual applications of these prediction tools may allow for an evidence-based standardization of outpatient shoulder arthroplasty patient selection.
In our study, one patient had an isolated DVT, one patient had a DVT/PE requiring readmission, one patient had an axillary nerve stretch injury, and one patient had an UGIB requiring readmission and transfusion. Rates of symptomatic and asymptomatic DVT after shoulder arthroplasty range from 0.09% to 13%, and rates of PE range from 0 to 3% [47]. Rapp et al. [47], based on a review of VTE after shoulder arthroplasty, recommended that mechanical prophylaxis be considered in all patients, and that chemical prophylaxis be considered on a case-by-case basis. Iatrogenic axillary neuropraxia following TSA was reviewed by LiBrizzi et al. [48], who reported that the rate of axillary nerve injury following TSA and RTSA ranged from 0% to 16% . The most common cause of axillary nerve injury is stretch, either due to intraoperative positioning of the arm or retractor use for visualization [48]. All cases observed by LiBrizzi et al. [48] were neurapraxias that resolved completely following observation. One of our patients also experienced complete neurologic recovery at 9 months postoperatively following observational management. Lastly, we reported one case of UGIB requiring readmission and transfusion. No prior study has specifically described the incidence of UGIB following TSA; however, rates of UGIB following hip and knee arthroplasty have been reported to be as high as 4.5% [49-51]. Risk factors include preexisting peptic ulcer disease, advanced age, smoking, and use of steroids, NSAIDs, and anti-coagulation [49]. Our patient had several risk factors: she had peptic ulcer disease and was on clopidogrel, was allergic to NSAIDs, and did not take any perioperatively.
Strengths of our study are that we reported 90-day postoperative complication and readmission rates following inpatient and outpatient TSA with a nonspherical humeral head and an inlay glenoid, which have not previously been reported. One hundred eighteen patients where included, which is the largest relative cohort to receive this TSA prosthesis to date. However, 118 patients is relatively small in comparison to the number of patients evaluated in studies that have investigated traditional TSA, RTSA, and HA. Additional patient recruitment and follow-up are therefore warranted.
Limitations of our study include that only 16 surgeries were performed in the free-standing ASC setting; more patients are needed to adequately power a comparison between inpatient, outpatient hospital-based, and free-standing ASC surgeries. Once TSA in the freestanding ASC is approved by the CMS, the proportion of procedures performed there will likely increase. The aim of this study was to assess the safety of outpatient TSA with humeral head and inlay glenoid replacement, therefore no functional patient-reported outcomes or long-term complication rates were included; however, both are topics for future study as we continue to follow this cohort. Inpatient and outpatient groups were not age- or comorbidity-matched cohorts, with the outpatient group being younger and healthier. Patients who underwent outpatient procedures were selected for that surgical setting based on preoperative anesthesia and surgeon evaluation. These preoperative differences may have impacted the outcomes in the study given that age and comorbidities increase postoperative complications. Thus, we cannot interpret our results to mean that outpatient TSA with a nonspherical humeral head and inlay glenoid is applicable to all patients; our study only provides evidence that TSA with a nonspherical humeral head and inlay glenoid is safe for patients selected for outpatient surgery based on our preoperative anesthesia and surgeon evaluations.
CONCLUSIONS
In this study, TSA with a nonspherical humeral head component and an inlay glenoid was performed with low short-term complication and readmission rates of 3.4% and 1.7%, respectively. Inpatient and outpatient TSA procedures were both performed safely with no difference in complications or readmissions between surgical settings.