Effect of cigarette smoking on the maintenance of reduction after treatment of acute acromioclavicular joint dislocation with hook plate fixation
Article information

Abstract
Background
The purpose of this study was to determine the association between smoking and clinical outcomes of hook plate fixation for acute acromioclavicular (AC) joint injuries.
Methods
This study retrospectively investigated 82 patients who underwent hook plate fixation for acute AC joint dislocation between March 2014 to June 2022. The patients were grouped by smoking status, with 49 in group N (nonsmokers) and 33 in group S (smokers). Functional scores and active range of motion were compared among the groups at the 1-year follow-up. Coracoclavicular distance (CCD) was measured, and difference with the uninjured side was compared at initial injury and 6 months after implant removal.
Results
No significant differences were observed between the two groups in demographic factors such as age and sex, as well as parameters related to initial injury status, which included time from injury to surgery, the preoperative CCD difference value, and the Rockwood classification. However, the postoperative CCD difference was significantly higher in group S (3.1±2.6 mm) compared to group N (1.7±2.4 mm). Multivariate regression analysis indicated that smoking and the preoperative CCD difference independently contributed to an increase in the postoperative CCD difference. Despite the radiographic differences, the postoperative clinical outcome scores and active range of motion measurements were comparable between the groups.
Conclusions
Smoking had a detrimental impact on ligament healing after hook plate fixation for acute AC joint dislocations. This finding emphasizes the importance of smoking cessation to optimize reduction maintenance after AC joint injury.
Level of evidence
III.
INTRODUCTION
Due to the increasing popularity of recreational activities and sports, the prevalence of acromioclavicular (AC) joint injuries is on the rise [1]. Neglected injuries can lead to chronic pain, instability, and decline in shoulder function [2,3]. Various surgical approaches including the use of Kirschner wire, hook plate, and cortical button have been employed to stabilize the AC joint [4-7]. Among them, the clavicular hook plate is anatomically contoured to fit the clavicle and features a tapered hook designed to function as a lever beneath the acromion [8]. This lever action depresses the clavicle, promoting healing of the AC and coracoclavicular (CC) ligaments [9].
Although achievement of rigid fixation and early range of motion (ROM) are advantages of hook plate fixation leading to satisfactory clinical results, complications such as subacromial impingement, bony erosion, and peri-implant fracture have been noted [10-13]. As a result of these considerations, the implant is typically removed after 3 to 4 months of initial surgery. Following plate removal, it is common for the CC distance to remain similar to that of the unaffected side. However, in some cases, the CC distance reverts to the height prior to surgery [14-17]. Various reasons can contribute to inadequate healing, including that AC joint injuries predominantly occur in young, active male patients, many of whom are also active smokers [18,19].
Smoking has a detrimental effect on the outcomes of many orthopedic treatments. Among them, procedures requiring ligament and tendon restoration, such as anterior cruciate ligament reconstruction, rotator cuff repair, and lateral ankle ligament reconstruction, have been reported in numerous studies to be adversely affected by smoking [20-24]. Likewise, considering the importance of tendon healing, it is conceivable that smoking may also adversely affect AC joint injuries. However, as of our current understanding, no study has specifically investigated the relationship between smoking and AC joint injuries.
Therefore, the purpose of this study is to determine the association between smoking and clinical outcomes of hook plate fixation for acute AC joint injuries. We hypothesized that smoking would adversely affect AC and CC ligament healing, leading to loss of reduction and unfavorable consequences for patient outcomes.
METHODS
The Institutional Review Board of Severance Hospital at the Yonsei University College of Medicine approved this study (No. 4-2023-0858), and the requirement for informed consent was waived.
This study retrospectively reviewed the data of 112 patients who had undergone hook plate fixation for acute AC joint dislocation at our institution between March 2014 to June 2022. The inclusion criteria were (1) acute Rockwood type III or V AC joint dislocation and (2) minimum 1-year follow-up after the initial surgery. Exclusion criteria were (1) fixation method other than the hook plate, (2) peri-implant complication requiring further surgical intervention such as clavicle fracture, (3) a previous history of surgery on the affected shoulder, (4) concomitant fracture of the ipsilateral shoulder, (5) former smoker (quit smoking before the surgery or during the follow-up period), and (6) individuals with a worker’s compensation claim. Overall, 82 patients were included in this study (Fig. 1). Smoking status was documented preoperatively at hospitalization and was updated on outpatient visits. Duration and quantity of smoking were obtained, and individuals who had smoked more than 100 cigarettes in their lifetime and currently smoked on a regular basis were defined as “smokers” [25]. “Nonsmokers” were defined as individuals naïve to exposure of tobacco.
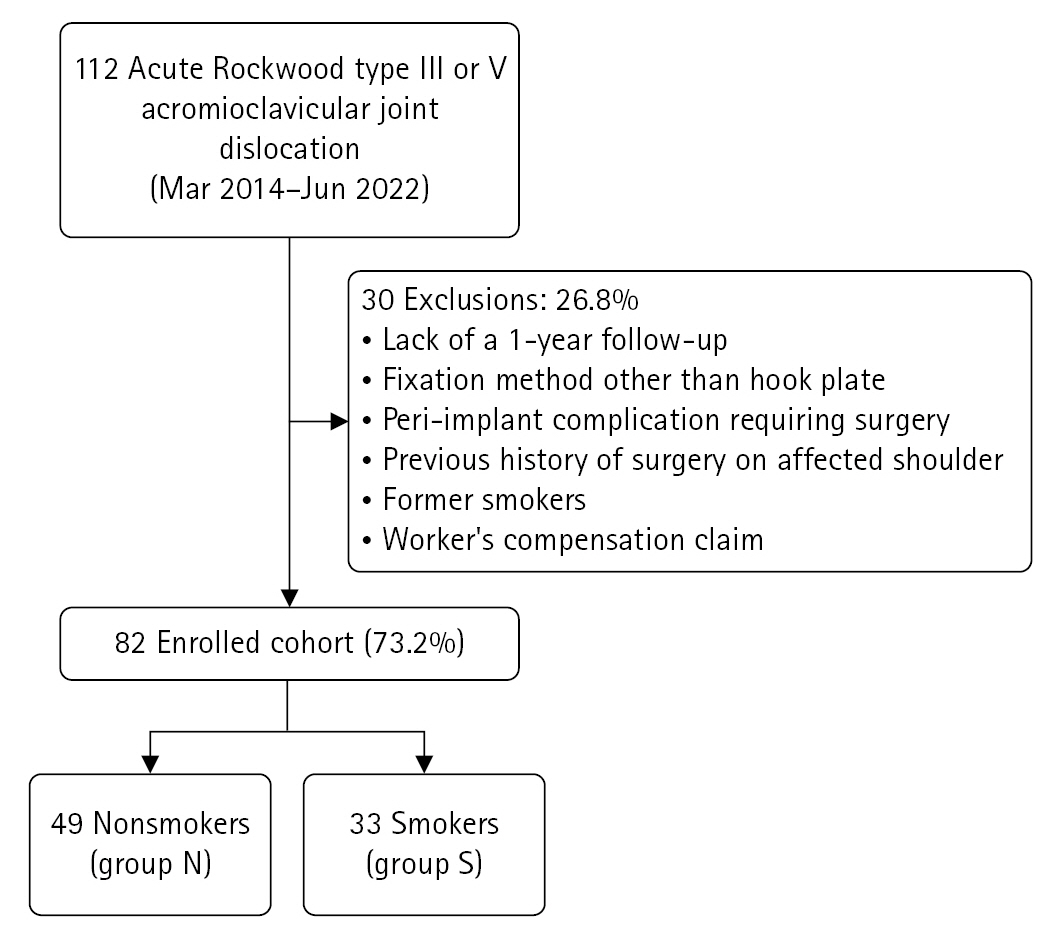
Consolidated Standards of Reporting Trials (CONSORT) flow diagram presenting the flow of patients across the study.
Surgical Procedure and Postoperative Rehabilitation
All surgical procedures were performed by two experienced orthopedic surgeons with expertise in shoulder surgery. The surgery was conducted under general anesthesia in the 20º beach chair position. A 7- to 8-cm-sized skin incision was made over the distal clavicle and AC joint, positioned one-fourth of the width from the posterior border of the clavicle. The AC joint was identified, and the hook component was passed through the posterior aspect of the AC joint under the acromion, while the locking plate component was placed on the distal clavicle (3.5 mm LCP clavicle hook plate, Synthes). The plate’s contour and reduction status were carefully examined under fluoroscopic guidance. The depth of the hook was determined using the contralateral AC joint radiograph as a reference, and slight over-compression was intended. If there was a sufficient amount of ligament remaining, the ruptured AC ligament was repaired after hook plate fixation. After achieving satisfactory reduction, locking screw fixation and secure deltotrapezius fascial repair were performed over the plate. Self-assisted circumduction exercises were initiated the day after surgery, as tolerated. Following 2 weeks of immobilization of the operated arm, self-assisted active ROM exercises were initiated. Radiographic follow-up was conducted on a monthly basis, and plate removal was performed at 3 to 4 months postoperatively.
Clinical and Radiological Assessments
Medical records were reviewed for patient demographics and clinical factors. The demographic factors were age, sex, time from injury to surgery, and duration from hook plate fixation to implant removal. Functional outcomes were evaluated using the visual analog scale and the subjective shoulder value. Active ROM was measured, including forward flexion in the scapular plane, external rotation with the elbow at the side, and internal rotation. Internal rotation was quantified by assigning scores to the highest spinal vertebra level reached by the patient's thumb during internal rotation. T1 to T12 were scored from 1 to 12, L1–L5 were scored from 13 to 17, and the sacrum was scored 18 [26-28]. The active ROM and functional scores were assessed during every follow-up by an independent examiner who was blinded to group assignment and patient information.
Both clavicle anteroposterior views were acquired preoperatively and then monthly after surgery. Initial radiographs were used for measuring the coracoclavicular distance (CCD) and classifying the patients according to the Rockwood classification. The CCD was defined as the perpendicular distance from the highest point of the coracoid cortex to the lower margin of the clavicle cortex. The CCD was assessed in comparison with the contralateral shoulder 6 months after implant removal to ascertain the extent of reduction maintenance (Fig. 2). Two shoulder-specialized orthopedic fellows participated in the CCD measurement, and the mean values were subjected to analysis.
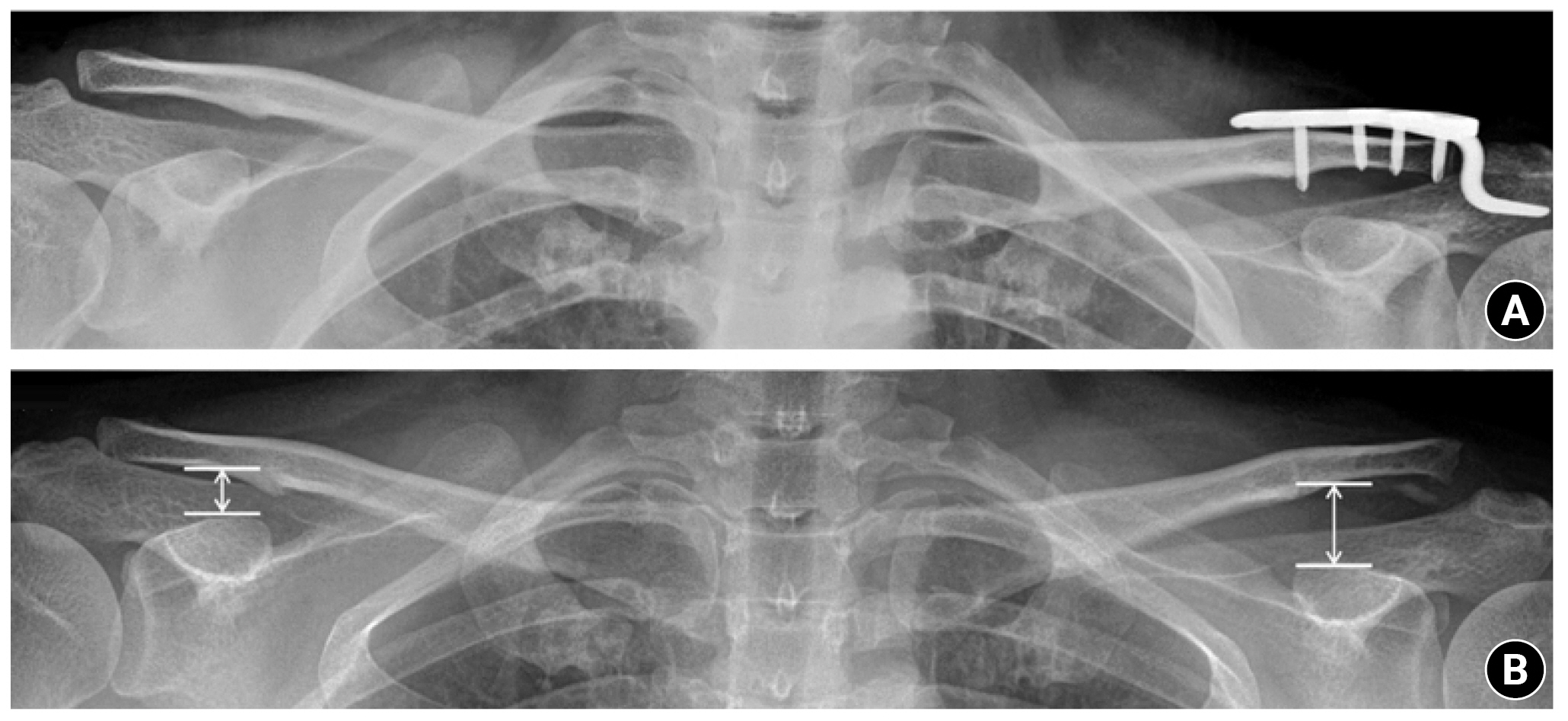
Anteroposterior radiograph of a patient treated with hook plate fixation for an acromioclavicular joint injury. (A) Hook plate fixation with intentional over reduction. (B) Six months after implant removal. The coracoclavicular distance was defined as the perpendicular distance from the highest point of the coracoid cortex to the lower margin of the clavicle cortex.
Statistical Analysis
Statistical analyses were performed using SPSS software ver. 25.0 (IBM Corp.). Student t-test was used to compare continuous variables between the groups, and chi-square test was used for categorical values. Reduction maintenance status according to CCD difference was determined, and univariate regression analysis was performed. Variables with statistically significant differences were subjected to multivariate regression analysis via a stepwise method. A significance level of P<0.05 was used with a 95% confidence interval.
RESULTS
Patient Demographics
A total of 82 individuals was enrolled in the study, 49 in group N (nonsmokers) and 33 in group S (smokers), with an average smoking history of 17.6±15.9 pack-years for the smokers. There were no significant differences between the two groups in terms of demographic factors, including age, sex, time from injury to surgery, and duration from hook plate fixation to implant removal.
Clinical and Radiological Outcomes
There were no notable differences in the parameters related to initial injury status such as the preoperative CCD difference and the Rockwood classification. However, the postoperative CCD difference (the CCD difference at 6 months after plate removal) was significantly higher in group S (3.1±2.6 mm) compared to group N (1.7±2.4 mm) (Table 1). No discernible difference in the clinical scores and active ROM were discovered between the two groups, except for internal rotation (Table 2). Univariate regression analysis was conducted using the postoperative CCD difference as the dependent variable, and smoking status and preoperative CCD difference were identified as the significant factors. Furthermore, as confirmed by multivariate regression analysis, both factors independently influenced the postoperative CCD difference (Table 3). Among the patients in group S, two experienced chronic pain associated with reduction loss and underwent CC ligament reconstruction.

Demographic characteristics

Functional scores and active range of motion between groups

Uni- and multivariable regression analysis of postoperative CCD in the affected shoulder
DISCUSSION
The primary finding of this study is that smoking has a detrimental effect on ligament healing in patients with acute AC injury. Despite differences in radiographic parameters, the two groups exhibited comparable patient-reported clinical outcome scores and ROM. Furthermore, regression analysis established smoking and the initial CCD difference as independent risk factors for increase in the postoperative CCD difference.
Hook plate fixation has been recognized as a straightforward procedure with satisfactory clinical outcomes for treating acute AC joint dislocation [17,29]. Ko et al. [30] conducted a long-term outcome comparison between hook plate fixation and the suture button fixation technique. The study did not find significant differences in terms of functional outcome scores, final CCD, or complications between the two treatment groups. Therefore, both treatments were concluded to be viable and effective options for addressing AC joint dislocation. Suture button fixation does not require a second surgery for device removal, and the retained suture loop prevents further displacement, facilitating ligament healing over a longer period of time. On the contrary, for hook plate fixation, removal is necessary, which emphasizes the importance of achieving satisfactory ligament healing before plate removal. Unlike degenerative shoulder conditions such as rotator cuff tears, AC joint injuries are common among young, active male patients with a high prevalence of smoking, as evidenced by our cohort, where smoking was observed in 36% of the cases [18,19]. While smoking is well known to adversely affect ligament healing [31,32], the specific impact of smoking on healing of the ligaments after hook plate fixation for AC joint injury remains uncertain. For this reason, we initiated this study.
Reduction loss associated after hook plate removal has been reported in the literature. In a recent retrospective study of 118 patients by Lee et al. [33], risk factors for reduction loss after hook plate fixation were identified as female sex, delayed time to surgery (>7 days), and the initial coracoid clavicular displacement ratio. The initial CCD reflects the degree of damage to the soft tissue surrounding the AC joint and was found to affect reduction loss, aligning with our results. On the other hand, the duration to surgery and female sex did not significantly affect the postoperative CCD difference in our cohort. This may be because most patients (80.4%) underwent treatment within 1 week, and only five female patients were enrolled, attenuating the impact on the outcome.
Our study is focused on establishing the effect of smoking on the outcome of hook plate fixation, and we observed an increase in the postoperative CCD difference related to smoking. Smoking is recognized for its adverse impact on the outcomes of orthopedic procedures involving ligament healing. Unfavorable outcomes, such as increased anterior translation, as well as significantly low subjective and objective clinical scores, have been found to be related to smoking in anterior cruciate ligament reconstruction [20]. Park et al. [23] performed a propensity score matched analysis to determine the effect of smoking on healing of rotator cuff tears after arthroscopic repair. They noted higher retear rates in smokers (29.4%) compared to nonsmokers (5.9%), confirming the association between smoking and compromised rotator cuff healing. Studies have shown that smoking hinders normal regeneration of musculoskeletal tissue, impairing microvascular flow and disrupting the balance of bone and collagen metabolism [34,35]. Nicotine, the main component of tobacco, impedes cell proliferation, vascular ingrowth, and collagen formation [32,36,37]. Additionally, carbon monoxide and hydrogen cyanide, along with nicotine-induced vasoconstriction, further contribute to tissue hypoxia and delay the healing process [38,39]. Based on these research findings, it is essential to emphasize the importance of smoking cessation to patients considering hook plate fixation for acute AC joint injuries.
In the current study, smoking status did not result in a statistically significant difference in clinical outcomes, such as ROM and functional score, except internal rotation. Smoking is recognized for its potential to cause synovial inflammation and contributes to the onset of stiff shoulder, which can explain the difficulty in internal rotation according to our study [40]. Although our findings are based on a short-term follow-up period, the negative effect of smoking on radiographic CCD maintenance did not lead to discernible differences in clinical outcomes. Furthermore, considering that one point in internal rotation scoring is equivalent to the height of one vertebral body, the actual clinical significance may not be substantial. Similarly, the findings of Lee et al. [33] acknowledge that the loss of reduction did not exert a significant influence on short-term clinical outcomes during the 1-year follow-up. Nevertheless, two patients in the smoker group required additional CC ligament reconstruction due to chronic pain, and different conclusions may arise from longer-term studies.
There were several limitations to this study. First, it was a retrospective study with non-randomized patient assignment, which had the potential for selection bias. Second, the study was conducted with a small sample size. Conducting a multi-center study with a larger number of patients will likely provide more precise insights into the risk factors contributing to the reduction loss. Finally, the exact CCD measurement may have varied on the plain radiographs depending on the observers and the angles of radiograph acquisition.
CONCLUSIONS
Smoking was found to have a detrimental impact on ligament healing after hook plate fixation for acute AC joint dislocations. This finding emphasizes the importance of smoking cessation to optimize reduction maintenance after AC joint injury.
Notes
Author contributions
Conceptualization: THY. Data curation: YMC, THY. Formal Analysis: THY. Investigation: THY. Methodology: JHC, THY. Project administration: THY. Resources: THY. Software: THY. Supervision: YMC, THY. Validation: JHC, THY. Visualization: JHC, THY. Writing – original draft: JHC, THY. Writing – review & editing: THY.
Conflict of interest
Yong-Min Chun is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
Funding
None.
Data availability
Contact the corresponding author for data availability.
Acknowledgments
None.