INTRODUCTION
Shoulder pain is a common complaint in the general population, with a prevalence of 7%–27% that increases with age [1]. Of these cases, approximately 20% are caused by osteoarthritis (OA) of the acromioclavicular (AC) joint. An arthroscopic distal clavicle resection (aDCR) is an established and effective treatment after other non-operative treatments have failed [2,3]. It is essential to be able to distinguish if the shoulder pain is a product of AC OA or of concomitant pathologies, as multiple studies have reported that up to 93% of patients ≥30 years old demonstrate asymptomatic radiographic AC OA [4-6].
Physical examination tests to distinguish between AC pathology and other shoulder pathology, such as the Bell van Riet or the O’Brien, are not reliable enough in this patient population [7-11]. Krill et al. [12] suggested that AC injections be implemented as a diagnostic tool to differentiate between symptomatic AC OA and radiographic asymptomatic AC OA. Several studies have investigated the diagnostic value of a preoperative AC injection. However, none have observed a significant difference in outcome [13,14]. Some physicians have reported a distinction in aDCR outcome between patients who reported a good analgesic reaction to an AC injection compared to patients who reported a minimal positive reaction to an AC injection.
To the authors’ knowledge, no prior studies have investigated the difference in aDCR outcome between patients who reported a good analgesic reaction to an AC injection compared to patients who reported a minimal positive reaction to an AC injection. A significant difference would suggest that AC injections can differentiate between patients with symptomatic radiographic AC OA, for whom aDCR is beneficial, and asymptomatic radiographic AC OA patients, for whom aDCR is not beneficial.
The primary aim of this study was to determine the diagnostic value of a preoperative AC injection in discriminating between symptomatic and asymptomatic radiographic AC OA based on aDCR outcomes. It was hypothesized that patients with a good analgesic reaction to an AC injection would have a higher level of satisfaction with the aDCR compared to patients with a minimal analgesic reaction to an AC injection.
METHODS
The study was approved by the Institutional Review Board of Spaarne Gasthuis (No. 2022.0078). Informed consent was obtained from all included patients in this study.
Study Design
A single surgeon’s registry was reviewed to retrospectively identify patients who received aDCR for AC OA and a preoperative ultrasound- or radiographic-guided AC injection between January 2017 and October 2021. This study retrospectively reviewed cross-sectional, midterm data evaluating patient satisfaction, shoulder pain, and shoulder function. Patients were included if they were diagnosed with AC OA that was confirmed by physical examination and radiographic imaging and/or magnetic resonance imaging, according to the Claes Petersson grading system [15] and who had undergone ultrasound imaging to exclude any additional shoulder pathology. Patients were excluded if they had a history of prior surgery to the affected AC joint, had other diagnosed shoulder pathologies in the affected joint, had received AC injection elsewhere than the hospital at which this study was conducted, or had undergone an aDCR combined with a concomitant procedure (e.g., subacromial decompression according to Neer [16] or biceps tenotomy or cuff repair).
Surgical indications for aDCR were patients with clinically symptomatic and radiographic AC OA. Radiographic AC OA was diagnosed based on the “Zanca” view of radiographic imaging. AC OA was symptomatic if patients reported complaints of pain located in the AC joint and a high painful arc (150°–180°) along with at least one positive AC-specific physical examination test (e.g., the cross-over adduction test [17], the test of O’Brien [18], or the Bell van Riet [11]).
AC Injection
Patients received a minimum of one preoperative AC injection (standardized dosage: 1 mL of 1 mg/mL of lidocaine with 1 mL of 40 mg/mL Kenacort), and some patients received more than a single AC injection. All AC injections were administered under the guidance of ultrasound or radiographic imaging because multiple prior studies have shown that guided AC injections are more accurate and result in a significantly higher degree of pain reduction [7-10]. With an ultrasound probe, the AC joint was identified in the transverse plane, perpendicular to the clavicle. The injection was administered in-plane with the probe by an experienced nurse practitioner.
Surgical Technique
All surgeries were performed by the senior author (AVN). Patients were placed in a semi-Fowler beach chair position with the operated arm in length traction. A needle was used to locate the AC joint. The joint was initially inspected through the posterior portal. Using an inside-out technique, a second, anterosuperior portal was created. A partial bursectomy was performed to examine the bursal side of the rotator cuff. Thereafter, the distal segment of the clavicle was removed through the anterosuperior portal using an oval bur. Additionally, any osteophytes were removed on the inferior side of the clavicle or acromion with the bur. Patients were discharged on the same day and were motivated to immediately begin exercise therapy under the supervision of a shoulder physiotherapist. All patients were observed 6 weeks postoperatively.
Data Collection
Patients were digitally approached for participation in this study, and a questionnaire was sent to those who agreed. Non-responding patients were contacted by telephone to inquire if they had received the invitation e-mail after one week. The patients who were unable to complete the questionnaire digitally were interviewed over the telephone by a researcher (RJMV).
The baseline patient-reported outcome measures (PROMs), which include the Oxford Shoulder Score (OSS), the Subjective Shoulder Value (SSV), and the Numerical Rating Scale (NRS), and the patient characteristics (age, time to follow-up, sex, body mass index, lateralization of AC OA, left- or right-handedness, number of injections, success of AC injection, additional preoperative treatments, and postoperative complications and reoperation) were obtained from medical files. Data regarding the AC injection were routinely documented after administration and then once more 6 weeks later during a consultation by telephone. Postoperative PROMs were collected using a questionnaire. Due to inclusion of patients between January 2017 and October 2021, these PROMs represented patients who were one to 5 years postoperative.
Based on the patients’ reaction to the AC injection, the patient was either categorized into the good or minimal reaction group. A good reaction was defined as a minimum of 7 consecutive days of pain reduction following the injection. It was hypothesized that if 7 days of consecutive pain reduction occurred, pain derived from the AC joint could be assumed. A minimal reaction was defined as no pain relief or recurring pain within 7 days of the injection.
Outcomes
An analysis of PROMs, including patient satisfaction, OSS, SSV and NRS both at rest and during activity, was performed [19-22]. Patient satisfaction was addressed using two anchor questions: “What is the level of satisfaction with the overall function of the operative shoulder on a five-point Likert scale?” and “Would you have undergone the surgery knowing that the current state of your shoulder would be the outcome of the surgery?” (yes, no). Based on data from the OSS query, a report on specific individual activities was analyzed regarding the effort required to perform daily tasks. All data were collected using a data management system: Research Manager (Cloud9 Software B.V.).
Statistical Analysis
All analyses were performed using the IBM SPSS ver. 26.0 (IBM Corp.). Means and standard deviations for normally distributed data or medians and interquartile ranges (IQRs) were used for non-normally distributed data. Categorical variables are presented as numbers with accompanying proportions. The difference in reaction to the AC injection was tested with a Fishers’ exact test. Differences in PROMs were evaluated using Mann-Whitney U-tests and Wilcoxon’s signed-ranks tests. Sample size calculation was not performed due to the explorative nature of this study and the limited expected sample size. A P-value <0.05 was considered statistically significant.
RESULTS
Baseline Characteristics
In all, 51 patients were contacted. Forty-eight patients (94%) agreed to participate. Their mean age at surgery was 58.8±10.1 years. The cohort consisted of 46.0% male patients. Twenty-seven patients had a good reaction to the AC injection, and 21 patients had a minimal reaction to the AC injection (Table 1).
Patient-Reported Outcome Measures
Forty-six patients (96%) responded that they would undergo the surgery again knowing that the current state of their shoulder would be the outcome of the surgery. A median score of 4 of 5 (IQR, 4.0–5.0) was found when analyzing the patient level of satisfaction. No significant differences in the willingness to undergo the surgery again (P=0.861) or the level of satisfaction (P=0.234) were observed between patients who reported a good reaction or a minimal reaction to the AC injection (Table 2).
When comparing the baseline post-injection PROMs to the postoperative PROMs (median follow-up duration, 45 months; IQR, 31.0–52.8), the OSS (33.0–19.5, P<0.001) and SSV (50.0–90.0, P<0.001) improved significantly. Additionally, the NRS at rest (6.0–1.0, P<0.001) and during activity (8.0–2.0, P<0.001) also improved significantly (Table 3).
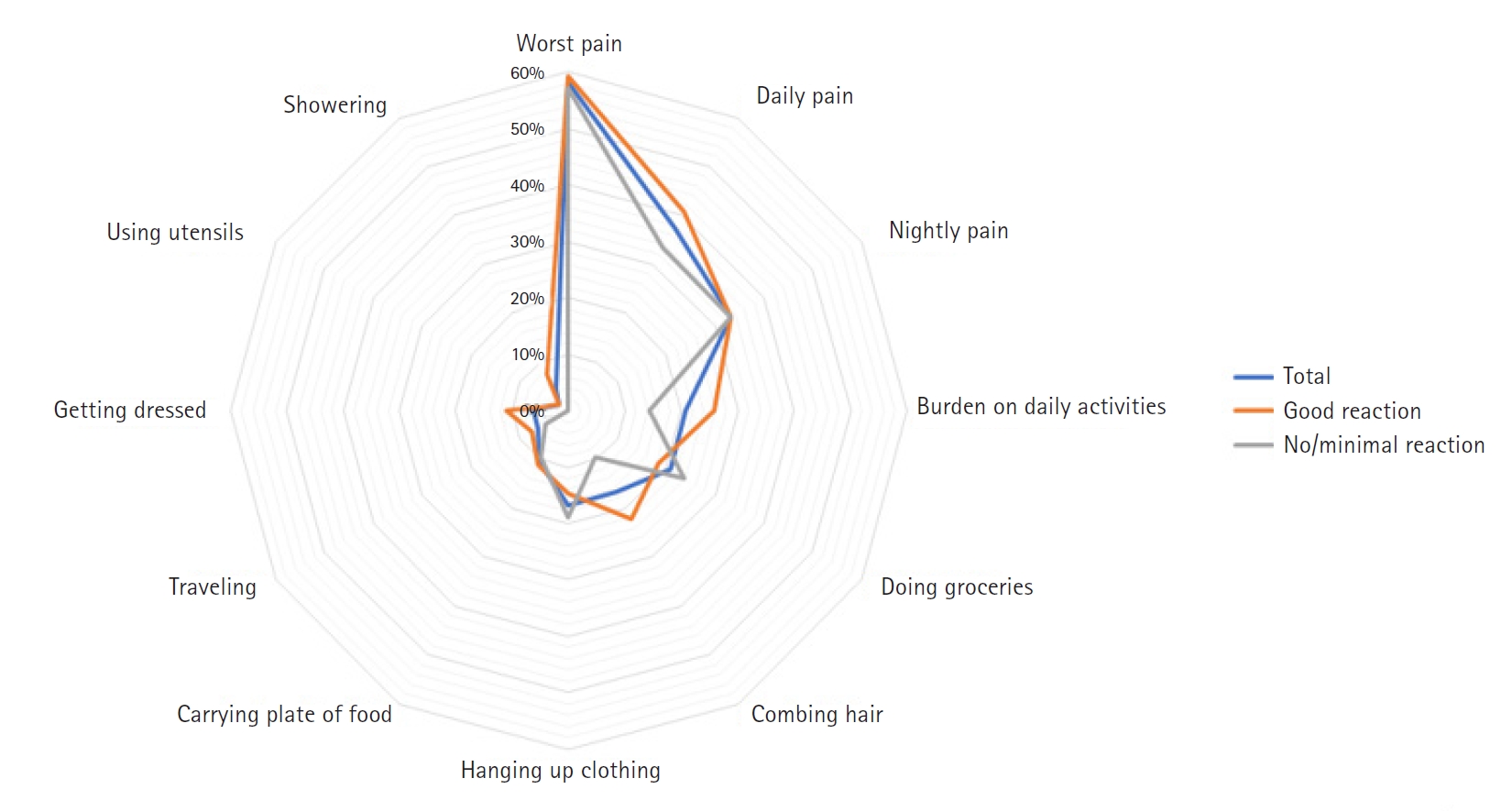
No significant differences in OSS, SSV, and NRS scores at rest or during activity were observed when comparing patients who reported a good reaction or a minimal reaction to the AC injection (P=0.612, P=0.641, P=0.684, and P=0.422, respectively) (Table 4). A few patients experienced difficulties carrying out daily activities, such as showering (4%), using utensils (2%), getting dressed (6%), or travelling (6%). Many patients reported daily (38%) and nightly (33%) postoperative pain. Activities such as shopping for groceries or combing hair were proven to be challenging, with 21% and 17% of patients scoring these tasks as having a medium to extreme difficulty level, respectively (Fig. 1).
DISCUSSION
The principal finding of this study was that patients were highly satisfied with the aDCR for AC OA, which had no relationship to the patients’ reaction to the AC injection. No significant differences in patient satisfaction or PROMs were observed when comparing patients who reported a good reaction to an AC injection and patients who reported a minimal reaction to an AC injection, which contradicted this study’s initial hypothesis.
Krill et al. [12] concluded that a combination of special tests for AC pathology was of limited diagnostic value due to a lack of specificity and suggested that ultrasound-guided AC injections may prove beneficial in discriminating between symptomatic and asymptomatic radiographic AC OA. However, this study did not provide evidence for the diagnostic value of a preoperative AC injection to make this distinction. The outcome of this study seemed to suggest that a distinction between symptomatic- and asymptomatic radiographic AC OA is unnecessary, as both patient groups were highly satisfied, and no differences in outcomes were observed.
The question remains why some patients reported a good reaction to the AC injection and other patients reported a minimal reaction, although all cases of AC OA were diagnosed in the same manner. Despite the physical examinations and imaging, a misdiagnosis of symptomatic AC OA might have caused this discrepancy, as research has shown that physical examinations may not be accurate in this population and lack specificity [7-11].
Literature regarding the success rate of AC injections is scarce, and only standardized shoulder function questionnaires (the University of California at Los Angeles [UCLA] shoulder rating scale) have been implemented. Our study was the first to implement the OSS score for AC OA, which provided more insight into postoperative shoulder function regarding daily activities. This study’s findings were in line with current literature, as Yang et al. [23] and Gokkus et al. [2] also concluded a significant improvement in shoulder function (UCLA) at the final follow-up. Regarding the OSS on an item level, shoulder function clearly improved postoperatively, although many patients retained a significant degree of pain (e.g., the percentage of patients who rated their daily pain as moderate to extreme was 38%). When combining these results with the significant improvement of NRS from baseline to postoperatively both at rest and during activity, it can be concluded that shoulder function had clearly improved, but shoulder pain did not fully subside. Our study was not the first to provide evidence for this discrepancy. Freedman et al. [24] corroborated these findings, stating that VAS scores improved significantly postoperatively, but 53% of patients retained some degree of pain. Direct postoperative pain may be caused by residual inflammation, granulation of scar tissue, or idiopathic nerve damage. However, these reasons do not explain why some patients retain long-term postoperative pain. OA pain remains poorly understood, but it is suggested that chronicity might affect the retainment of postoperative pain [25]. In patients with chronic OA pain, neuroplastic changes are seen in the peripheral and central nervous system. It has been hypothesized that the inhibition of successive pain stimuli is impaired in patients with chronic OA pain [26].
The strengths of this study consisted of the homogeneity of the study population, the high response rate, and the long follow-up period. Only three patients refused to participate, which produced a response rate higher than 94%. Our study aimed to evaluate midterm outcomes with a minimum of 12 months of follow-up. This study also had several limitations. First, because the success of an AC injection played a role in the decision of some surgeons to perform an aDCR, a selection bias existed in our patient population. A surgeon will expectedly be more inclined to treat a patient with an aDCR when the patient has already had a good reaction to the AC injection. This bias could be a main reason why no significant association was detected in our study. Second, it was necessary in some patients to perform a partial debridement during aDCR to create a clear view of the AC joint. This debridement could have influenced the postoperative outcomes, but this effect could not be identified. Third, PROMs were subjected to a ceiling effect. However, all PROMs that were used have been widely validated. Finally, for the baseline OSS, only the accumulated score was registered, so it was impossible to use the baseline scores for individual items. This lack of pertinent information prevented us from comparing individual OSS items, which could have further deepened our analysis. For a definitive conclusion on the association between the success of an AC injection and a patient’s postoperative functional and pain outcomes, a larger, prospective cohort study should be conducted.