INTRODUCTION
Recurrent anterior shoulder instability (RASI) is a common shoulder condition encountered in the young active population. Arthroscopic Bankart repair continues to be the most commonly performed surgery for RASI but has a high failure rate in the presence of critical bone loss [1]. The Latarjet-Patte procedure (LP) has an excellent track record of success for the treatment of RASI in the setting of critical glenoid and/or bipolar bone loss [2-5]. Through the transfer of the coracoid process and conjoint tendon to the anteroinferior glenoid, the LP exerts a triple stabilizing effect (bony, sling, and capsular effects) on the shoulder joint associated with high degrees of satisfaction and low recurrence rates in the long term [2,6,7].
Although the LP has seen an increase in its utilization in the past decade, arthroscopic Bankart repair still continues to be the most common procedure performed for RASI within the United States [3]. In recent years, the LP has seen an expansion in its indications to include treatment of failed arthroscopic capsulolabral repair (Bankart procedure) as a salvage procedure [8-12]. However, while outcomes of salvage LP have previously been reported, concern remains that outcomes may be suboptimal compared to those of the LP performed for unipolar/bipolar bone loss [9-12]. This is particularly evident by the recent work of Rodkey et al. [12] and Werthel et al. [11], with the latter reporting a greater incidence of re-dislocation in patients undergoing the salvage LP and the former reporting on greater levels of postoperative pain and lower functional outcome scores in patients who underwent an LP after arthroscopic repair.
Therefore, the purpose of this study was to compare the outcomes of LP for two different recurrent glenohumeral instability indications, primary instability surgery in the setting of critical bone loss (LP-BL) and salvage surgery performed for a failed primary arthroscopic Bankart repair (LP-FB). The primary outcome of this study was postoperative recurrence rate, and secondary outcomes included comparison of functional outcome scores and postoperative complications. We hypothesized that there would be no difference in clinical outcomes between these two groups. ŌĆā
METHODS
This study was approved by the Institutional Review Board of NYU Langone Health (No. s18-01216) and consent to participation in the study was obtained from patients. Patients who underwent an LP from 2017 to 2021 were identified from the senior authorŌĆÖs institutional database and consented to inclusion in our study.
Patient Selection and Cohort Classification
Patients were eligible for inclusion in our study if they met the following criteria: (1) underwent a primary LP for unipolar/bipolar bone loss or for failed arthroscopic Bankart repair, (2) were followed for a minimum of 24 months postoperation, and (3) were proficient in English to understand consent and participate in the study. Patients were excluded if they (1) underwent revision LP, (2) were non-English speakers, or (3) were not available for 24 months of follow-up. Patients were then separated into cohorts based on surgical indication: patients who underwent an LP to address unipolar or bipolar bone loss (LP-BL) and patients who underwent an LP after failed stabilization with arthroscopic Bankart lesion repair (LP-FB).
Data Acquisition
Preoperative data were extracted from electronic medical records via Epic (Epic Systems Corp.) independently by three trained clinical researchers. Metrics acquired included baseline patient demographics, shoulder range of motion (ROM), radiological imaging (radiographs, magnetic resonance imaging [MRI], computed tomography [CT] scans), and pre-operative clinical outcome scores in the form of patient-reported outcomes measurement information system (PROMIS) upper extremity (UE) computer adaptive test version 2.0, pain intensity, and pain interference.
Postoperative PROM data were acquired from patients at a minimum of 24 months postoperatively via surveys administered during office visits, over email, and by phone call. All patient data was stored within our institutional REDCap database (Vanderbilt University). This data consisted of PROMIS UE, PROMIS pain interference, PROMIS pain intensity, American Shoulder and Elbow Surgeons (ASES), and visual analog scale (VAS) pain scores. Shoulder ROM data was acquired at the latest follow-up during the physical exam. Additionally, patient records were screened by the clinical research team for any postoperative dislocation events and complications including but not limited to hematoma, infection (superficial and deep), neuropraxia (axillary and musculocutaneous), nonunion, graft/hardware failure, and the development of arthritis.
Radiological Analysis
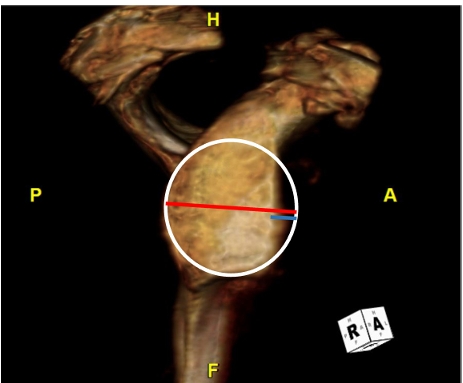
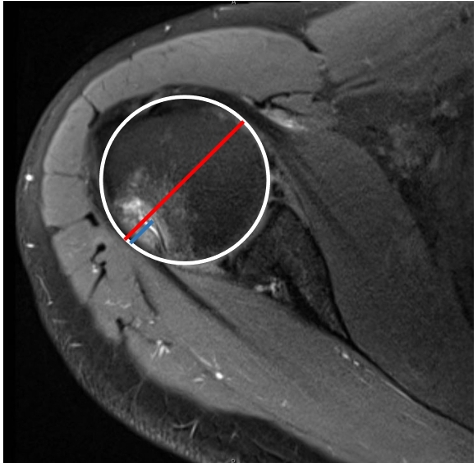
MRI and CT scans were available for analysis for 95% (45/47) of the patients in this study. Glenoid bone loss, Hill-Sachs lesion depth, and the presence of off-track/on-track lesions were determined for both groups by a fellowship-trained musculoskeletal radiologist (SG). The glenoid bone loss percentage was estimated using the circle method on the provided sagittal images as previously described (Fig. 1) [13]. Hill-Sachs depth was calculated by reviewing axial images and identifying the slice with the greatest degree of cortical impaction (Fig. 2). The depth was then estimated by a measurement taken between the impacted bone and adjacent circle margin. On-/off-track status was determined using previously described methods as well [13]. Postoperative radiographs were also acquired and evaluated for graft/hardware failure and screw displacement.
Surgical Technique and Rehabilitation
Patients in both cohorts underwent the LP in the beach-chair position under regional anesthesia (single-shot interscalene block) with few differences in the technique (described later). In brief, an 8-cm vertical incision was made from the coracoid toward the axillary fold. The cephalic vein was identified in the deltopectoral interval and was brought laterally with the deltoid. The clavipectoral fascia was incised, and the conjoint tendon was freed up distally. The coracoacromial ligament was transected in its entirety, leaving a stump of tissue of approximately 10 mm on the coracoid. The attachment of the pectoralis minor tendon was then released subperiosteally from the medial coracoid, and a soft tissue plane developed between the conjoint tendon and pectoralis minor distally.
A right-angled oscillating saw was used to perform coracoid osteotomy at the junction of the horizontal and vertical parts of the coracoid. The undersurface of the osteotomized coracoid was then decorticated and flattened with a saw or burr. Two drill holes (1 cm apart) were placed in the graft using a freehand technique. A horizontal subscapularis split was performed at the junction of the upper two-thirds and the lower one-third of the subscapularis. A T-shaped capsulotomy was then performed, exposing the inferior half of the glenoid rim. The damaged anterior labrum and capsule were removed, and the anterior glenoid neck was decorticated with a burr or osteotome from the 3- to 6-oŌĆÖclock positions (right shoulder).
In the LP-FB group, prior sutures and suture anchors were removed during the preparation of glenoid neck. Additionally, anterior glenoid rim fracture remnants were excised, if present, in both cohorts. The coracoid graft was then placed on the prepared surface of the glenoid neck and fixed with two screws. The stump of the coracoacromial ligament was repaired to the residual free capsular margin. A side-to-side repair of the subscapularis split was then performed, followed by a standard layered closure.
Postoperatively, a shoulder sling was used for the first 4 weeks, with pendulums and passive motion exercises beginning a few days after surgery. The subscapularis split, instead of a tenotomy, allows for the early introduction (2ŌĆō4 weeks) of isometric strengthening of the rotator cuff and active range of motion exercises of the shoulder. Most patients were allowed to return to sport-specific activities by 4 to 6 months.
Statistical Analysis
Statistical analysis was performed using SPSS ver. 28.0.1.0 (IBM Corp.). Quantitative data was expressed as mean and standard deviation, and qualitative data was reported as count and percentages. Descriptive statistics were calculated for both categorical and continuous variables. To compare internal rotation ROM, internal rotation scores were assigned as follows: no motion (0), motion to hip (1), motion to buttock/posterior superior iliac spine/sacroiliac joint (2), motion to the sacrum (3), motion to L4 to L5 (4), motion to L1 to L3 (5), motion to T8 to T12 (6), motion to T7 or above (7) as previously described [14]. Two-tailed independent samples t-tests were performed to compare continuous data, and FisherŌĆÖs exact test was conducted to compare categorical data. A P-value <0.05 was considered statistically significant.
RESULTS
Cohort Characteristics
Seventy-seven patients who underwent an LP from 2017 to 2021 were identified from the senior authorŌĆÖs database. Of that number, three patients underwent revision and were excluded from the study. Of the 47 that remained, 58 were eligible for 2-year follow-up, and 47 consented for inclusion into our study. As such, the total sample size of this study consisted of 47 patients (LP-BL: n=29 and LP-FB: n=18) with a mean age of 29.0┬▒11.4 years (range, 15ŌĆō58 years). For the overall sample, mean follow-up was 42.8┬▒14.5 months (range, 25ŌĆō79 months). There were no statistical differences in patient demographics between groups (Table 1).
Imaging Characteristics
The presence of glenoid bone loss and Hill-Sachs lesion depth were measured in 93% (27/29) of patients in the LP-BL group and 100% (18/18) of patients in the LP-FB group. The mean glenoid bone loss was 17.9%┬▒7% in the LP-BL group and 17.7%┬▒6.8% in the LP-FB group (P=0.921). The depth of the Hill-Sachs lesions was 4.4┬▒2.6 mm in the LP-BL group and 4.2┬▒ 2.6 mm in the LP-FB group (P=0.783). The presence of an off-track lesion was similar between groups: 41% in the LP-BL group and 38% in the LP-FB group (P=0.870).
Clinical Outcomes
Preoperative PROMIS scores were available for analysis in 78% (38/47) of patients, with 23 being in the LP-BL group (79%, 23/29) and 15 in the LP-FB group (83%, 15/18). There was a significant difference in pain intensity with respect to change in pre- to postoperative PROMIS scores (P=0.031) (Table 2). Postoperative PROMIS scores were acquired from 93% (44/47) of the patients. Postoperative VAS and ASES scores were acquired from 97% (46/47) and 91% (43/47) of the patients, respectively, with mean scores being reported in Table 2. Patients in the LP-FB group had statistically significantly lower VAS pain scores at the latest follow-up when compared to those of the LP-BL group (0.5┬▒1.1 vs. 1.94┬▒2.6, P=0.020). Of the patients available for physical exam (83%, 39/47), none reported significant deficits in ROM. Mean ROM for forward flexion, external rotation, and internal rotation are presented in Table 3.
Recurrence Rate and Complications
There were no significant differences in complication rates between the cohorts (LP-BL: 2/29, 6.9% vs. LP-FB: 2/18, 11.1%; P=0.629). Reported complications for the LP-BL cohort included re-dislocation and musculocutaneous neuropraxia, which resolved after 7 months, while the LP-FB cohort reported hematoma and superficial wound infection treated with antibiotics. There was no evidence of arthritic changes, graft failure, or screw failure (loosening, breakage, or displacement) as of the most recent radiographs.
DISCUSSION
The results of our study support our hypothesis demonstrating that the LP-FB cohort achieved upper extremity functionality that was comparable to that of their LP-BL counterparts. This study did not find history of arthroscopic Bankart repair to be a risk factor for a higher complication rate or suboptimal clinical outcomes as evidenced by no differences in 2-year complication or instability recurrence rates between the two cohorts.
Whether a history of failed arthroscopic Bankart repair increases the risk of instability recurrence and suboptimal clinical outcomes in patients undergoing LP remains controversial [10-12]. A retrospective study by Werthel et al. [11] analyzing long-term outcomes in 236 patients undergoing LP (20 LP-FB and 216 LP-BL) demonstrated significantly higher PROMs in the LP-BL cohort as measured by the Walch-Duplay (52┬▒25.1 vs. 72.2┬▒25.0, p<.001) and Simple Shoulder Test (9.3┬▒2.4 vs. 10.7┬▒1.9, P=0.001) scores. Similar results were reported by Flinkkil├ż et al. [10] in a retrospective analysis of 99 patients (52 LP-FB and 47 LP-BL) which demonstrated that LP-FB was associated with inferior outcomes as measured by mean Western Ontario Shoulder Instability scores (LP-FB: 76┬▒22 vs. LP-BL: 85┬▒15, P=0.02) and mean Subjective Shoulder values (LP-FB: 80┬▒18 vs. LP-BL: 88┬▒13, P=0.01) [10]. In contrast to the aforementioned studies, Yapp et al. [8] demonstrated no difference in outcome of LP when used as a primary or revision procedure for RASI. In a consecutive series of 205 patients (primary stabilization: n=145 and revision stabilization: n=60), the authors [8] found no differences in recurrence rate or complications between the two cohorts and demonstrated comparable outcomes for PROMs. Moreover, in our study, mean postoperative PROMIS scores fell within one standard deviation of the reference PROMIS T-score of 50┬▒10, indicating upper extremity functionality akin to that of the general populace of the United States [15].
In the current study, the LP-FB group had lower VAS pain scores at most recent follow-up when compared to the LP-BL group. In contrast to these results, Werthel et al. [11] demonstrated higher postoperative VAS pain scores in the LP-FB cohort (LP-FB: 2.6 ┬▒2.7 vs. LP-BL: 1.2┬▒1.7, P=0.01). Although these differences are statistically significant, they may not be clinically significant as they did not reach the minimal clinically important difference threshold of 1.7 in Werthel et al.ŌĆÖs study [11,15].
Perhaps the most important finding of this study was the lack of significant difference in the recurrence rate of dislocations between the LP-FB and LP-BL cohorts at 1-year follow-up, in agreement with most previous research [10-12]. However, a retrospective study by Rodkey et al. [12] investigating 2-year rates of recurrent shoulder instability proposed that the LP-FB was associated with significantly higher rates of dislocation (LP-FB: 20% vs. LP-BL: 9.1%, P=0.158) [12]. However, the population analyzed in that study was included in a military health system database and therefore predisposed to higher physiological demands compared to the general population, possibly limiting the external validity of the study.
While the present study lends evidence to the fact that LP can be used as a viable salvage/revision procedure with good functional outcomes, it would be remiss of us to not discuss the prevalence of complications surrounding its salvage indication. The overall complication rate of this study was 8.5% (4/47), consisting of neuropraxia, re-dislocation, hematoma, and superficial wound infection, all of which have been extensively documented post-LP [17,18]. Similar to a recent study evaluating short-term complications between the LP-FB and LP-BL, there were no statistically significant differences between complication rates between cohorts at 2 years postoperatively (P=0.63) [19].
Our study was not without limitations. First, the overall sample size was small, and there was unequal sample distribution between groups, with the LP-BL cohort being larger than the LP-FB cohort. However, this is likely reflective of the actual population, of which few patients undergo an LP following failed arthroscopic instability repair in the United States. Second, this is a short-term follow-up study with a mean follow-up period of 42.8 months. Third, we were unable to acquire information regarding return-to-play/sport data from our patients or feelings of subjective instability. Lastly, we were unable to collect preoperative ROM or PROMIS scores from all patients. Despite this limitation, the postoperative outcome scores were collected from >90% of patients and demonstrated good clinical outcomes.