Epithelioid hemangioma (EH) of bone is a rare vascular tumor that generally exhibits benign progression. It is currently classified as a benign vascular neoplasm in the most recent World Health Organization (WHO) classification [1]. However, rarity and histological similarity with other vascular tumors have led to diagnostic difficulties. Moreover, because of the locally destructive clinical presentation and the presence of atypical histologic features with infrequent mitotic activity and necrosis, EH is often misdiagnosed as low-grade malignant epithelioid hemangioendothelioma (EHE) or high-grade malignant epithelioid angiosarcoma (EAS) [2,3]. EH of bone occurs as a benign tumor, and the treatment and prognosis differ from those of other malignant hemangioma tumors. Therefore, diagnosis through imaging studies and histopathological examination is mandatory to determine the appropriate course of treatment. We report a rare case of EH occurring in the acromion of the scapula that was thoroughly treated with curettage of tumor.
As this is a case report of a single patient, there was no requirement for institutional review board review and approval. This case report was approved for exemption from the informed consent process as it was a retrospective analysis and report of clinical data (including pathological tissue and medical image data) obtained during the already completed treatment process.
CASE REPORT
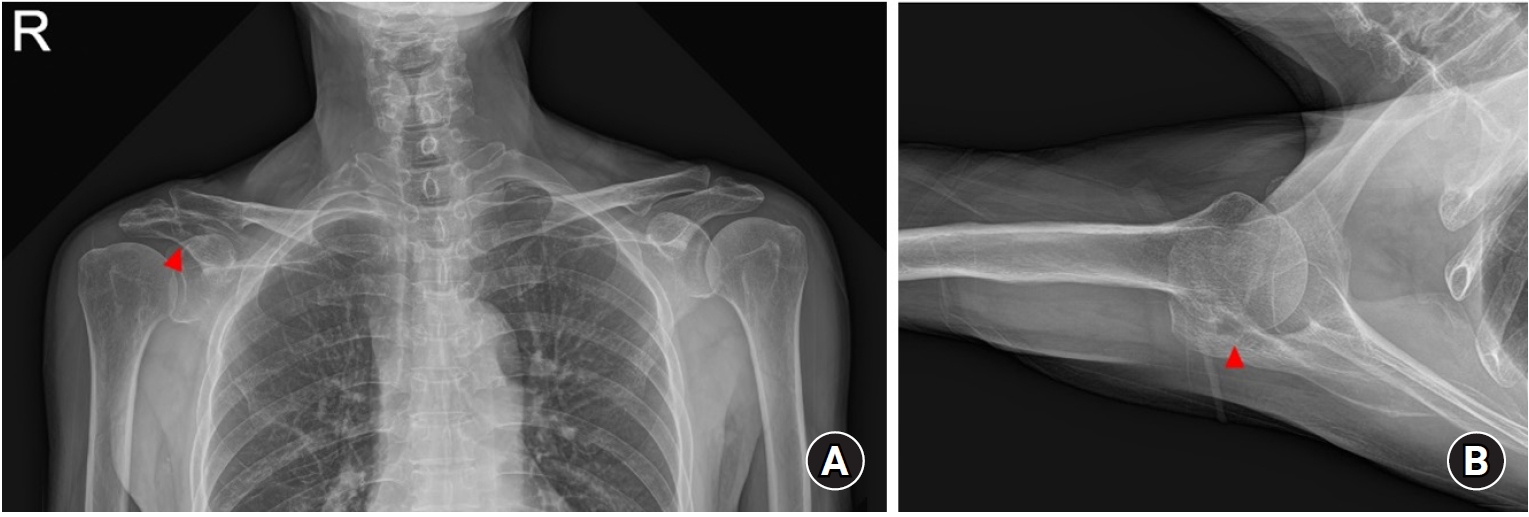
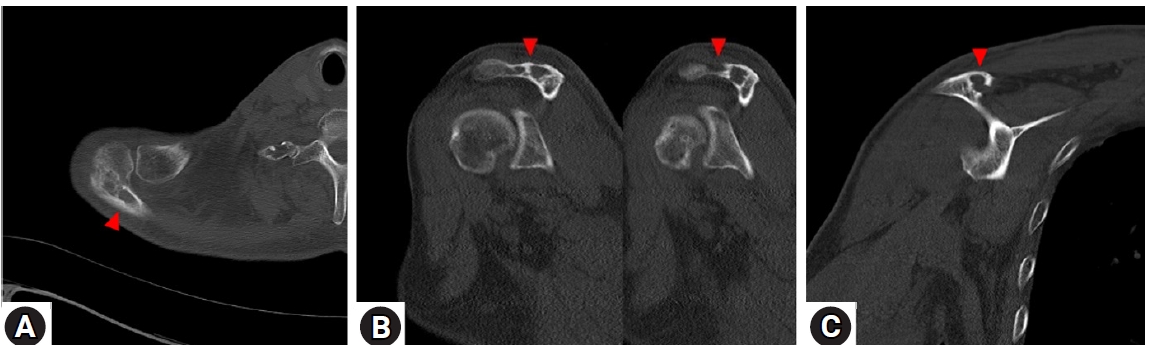
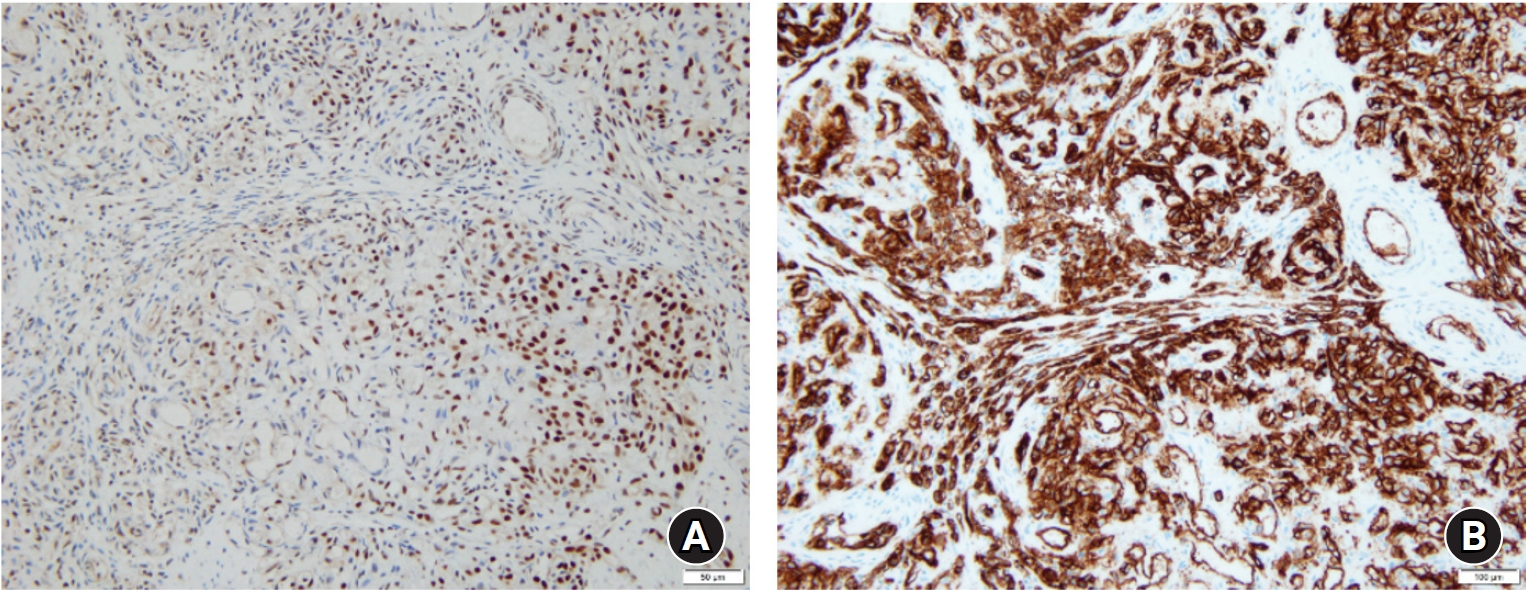
A 69-year-old man with no history of trauma presented with deteriorating sleep-disturbing right shoulder pain, which began approximately 1 year prior to presentation. The pain did not improve after prior non-steroidal anti-inflammatory drug use or several corticosteroid injections into the shoulder by a general practitioner. On clinical examination, the patient had full range of motion of the shoulder with signs of impingement. There was definite tenderness on the acromion, but no bruising, erythema, or warmth was noted. Laboratory examinations were unremarkable. Radiographs showed acromioclavicular (AC) joint space narrowing and an osteolytic lesion in the right acromion (Fig. 1). Subsequent computed tomography (CT) study showed a well-defined osteolytic lesion with multiple septations and cortical destruction of the posterior acromion and lateral end of the scapular spine (Fig. 2). Magnetic resonance imaging (MRI) confirmed the presence of a highly enhancing tumor occupying the posterior acromion and lateral end of the scapular spine, breaching cortices and infiltrating surrounding soft tissues (Fig. 3). A needle biopsy was performed. Histologically, the tumor had a lobular architecture, consisting of small, capillary-sized vessels. The epithelioid endothelial cells had a moderate amount of eosinophilic cytoplasm. Mitoses were relatively infrequent but not atypical. Intralesional hemorrhage or necrosis was not present. Immunohistochemically, the epithelioid endothelial cells had strong expression of FLI1 and CD34 but tested negative for HHV8 (Fig. 4). Based on these histopathological and immunohistochemical features, the patient was diagnosed with EH of the right scapula without any signs of malignancy. The lack of irregular inter-anastomosing vessels and malignant cytologic atypia, as well as the low mitotic rate, allowed distinction from angiosarcoma. Unlike EH, most EHEs do not show well-formed vascular channels and instead display anastomosing cords of cells with variable vacuolation and myxohyaline stroma.
The patient was treated with curettage of the lesion in the acromion and resection of the lesion in the surrounding soft tissues. After the procedure, the patient’s pain significantly improved. On the final, 2-year postoperative follow-up, enhanced MRI was performed to check for recurrence. The patient showed no recurrence and no surgery-related complications.
DISCUSSION
EH of the bone has been reported several times in the literature [2-8]. The diagnosis of EH, particularly in osseous locations, remains challenging because of its atypical histologic features being confused with other epithelioid vascular neoplasms such as EHE or EAS. According to the 2018 WHO classification, EH is classified as benign, while EHE and EAS are malignant [1]. Therefore, it is important to accurately distinguish EH from EHE and EAS owing to critical differences in clinical behavior and prognosis. EH of bone is usually solitary and rarely presents as multifocal lesions. It occurs most frequently in the metaphysis and diaphysis of long tubular bones of the extremities (40%), followed by the short tubular bones of the distal lower extremity (18%), vertebrae (16%), and small bones of the hands (8%) [4]. It has been observed in all age groups, with men affected slightly more frequently. The most common presenting complaints are pain and swelling of variable duration in the affected region. Radiographic features show well-defined margins with expansile growth, intralesional septae, radiolucent lytic or cystic-appearing lesions, and occasional cortical erosions and soft tissue extension [4-6]. Mixed osteolytic and sclerotic features on radiographs can be noted [5], and EH lesions are lucent and well marginated [6]. However, differential diagnoses based on these plain radiographic features are non-specific and can include giant cell tumor, aneurysmal bone cyst, and metastatic tumors. Similar to plain radiographs, CT shows well-defined, septate, expansile, lytic lesions with cortical destruction and bony expansion. T2-weighted MRI will usually show well-defined lesions that are isointense or slightly hyperintense relative to skeletal muscle. There is variable surrounding marrow edema and enhancement and sometimes cortical disruption with periosteal reaction [2,6]. Histologic features of EH include lobular proliferation of small, capillary sized vessels lined by large epithelioid endothelial cells with eosinophilic cytoplasm, infrequent mitoses, possibly small foci of necrosis, and stroma consisting of connective tissue sometimes with inflammatory infiltrates. Morphologically, it is difficult to distinguish between EH and EHE due to a considerable overlap at the pathological level, although EHE often shows infiltrative borders, arranges in clusters or cord-like structure, lacks inflammatory reaction, and often possesses myxoid or hyalinized stroma [2,6,9]. Although accurate assessment of lesional histologic features is of paramount importance for differential diagnosis of these epithelioid vascular neoplasms, expression of immunohistochemical markers and genetic abnormality must also be considered. Immunohistochemically, EHs express typical endothelial markers including CD31, CD34, FLI-1, and ER [2,6,9]. Staining for smooth muscle actin demonstrates the presence of surrounding pericytes. Several recent studies have shown recurrent genetic alterations in vascular tumors, such as FBJ murine osteosarcoma viral oncogene homolog (FOS) and FBJ murine osteosarcoma viral oncogene homolog B (FOSB) rearrangements in a subset of EH. Gene rearrangements in FOS and FOSB are present in 29% and 20% of EHs, respectively [7,10]. Differential diagnosis is challenging, but distinguishing this disease from other vascular neoplasms is important because of the diversity of indicated treatments [5,6]. Previous studies have suggested various methods for treating EH. Xian et al. [5] treated a patient with EH at the proximal radius and distal humerus with curettage and filling with cement. Nielsen et al. [6] used less invasive curettage or marginal en bloc resection of tumor mostly to treat EH successfully. Tsikopoulos et al. [8] treated a case of huge EH of the scapula with minimally invasive treatment using a combination of chemoembolization and microwave ablation. There is no consensus regarding the optimal treatment of EH. The current treatment options are curettage and bone grafting or en bloc resection. Local recurrence of EH or lymph node involvement is a rare complication after incomplete resection of the tumor. Xian et al. [5] presented a case of EH with multifocal metachronous bone lesion. There was controversy surrounding the cause of local recurrence, including distant metastasis or manifestation of multicentricity. Current researchers tend to consider EH a benign vascular tumor with metastatic potential [2,6]. Thus, careful follow-up should be performed even after symptom resolution. We decided to treat our patient’s tumorous condition with curettage based on its size and location on his predominant shoulder, especially as extensive surgical excision may cause functional impairment and complications in daily life. Curettage was followed for 2 years, during which there was no evidence of recurrence. The patient was satisfied with post-treatment pain relief.
In conclusion, we report a case of an EH of the acromion causing intractable shoulder pain with conservative care. This case was successfully treated with simple curettage without further recurrence or complication. Due to the metastatic potential of EH, careful follow-up for any complaint should be undertaken. Although it is a rare case of EH of the shoulder, EH familiarity and awareness can help pathologists make a correct diagnosis. Treatments may vary from patient to patient, depending on existing medical conditions or target location. However, due to its rather benign character, EH of bone should mostly be treated with curettage or marginal en bloc excision. As a rare disease entity that may present in various locations and sizes, EH should be further studied to create a proper treatment plan.