INTRODUCTION
Clavicle fracture is a common injury, with midshaft fractures accounting for about 80% of all clavicle fractures [1,2]. In the 1960s, Neer [3] and Rowe [4] reported a nonunion rate of 0.1–0.7% in conservatively treated midshaft clavicle fractures. Since then, most midshaft clavicle fractures have been treated effectively with conservative approaches using an arm sling or figure-of-eight bandage [5]. Recent studies have not reported significant differences in the functional outcomes between conservative and surgical treatments for displaced midshaft clavicle fractures. However, the nonunion/malunion rates have been significantly higher in patients treated conservatively [6-8], especially those with completely displaced midshaft clavicle fractures with a displacement of ≥100%, where a 15%–20% nonunion rate has been reported [9,10].
These recent long-term outcomes of increased nonunion/malunion rates after conservative treatment have changed the indications for surgery when treating midshaft clavicle fractures. However, if the long-term functional outcome is not significantly different between conservative and surgical treatments and both treatment methods provide good outcomes, other factors may also be needed to aid in decision-making. Because both treatment methods have their own pros and cons, clinicians must consider not only the long-term outcome of the treatment methods, but also the patient’s condition and the discomfort experienced at the time of injury or the expected satisfaction with the final outcome of the treatment. Further, shared decision-making after sufficient consultation between patient and surgeon can lead to better outcomes when selecting treatment plans for orthopedic conditions [11].
We wondered if any factors present at the time of injury were associated with the patient’s decision to proceed with surgical treatment. We also investigated if there were common characteristics among patients who were satisfied with their treatment method. The objective of this study was to investigate the hypothesis that patients with midshaft clavicle fracture with a displacement of ≥100% will eventually undergo surgical treatment and will be satisfied with the surgical treatment.
METHODS
All procedures performed in studies involving human participants were carried out in accordance with the ethical standards of the Institutional Review Board of Asan Medical Center (IRB No. 2018-1091), and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Patients and Study Design
We retrospectively reviewed the medical records of patients who were diagnosed with a midshaft clavicle fracture in the outpatient clinic and emergency department of Asan Medical Center in Seoul, South Korea, between March 1, 2013 and December 31, 2014.
During the eligibility period, we identified 81 patients from 19 to 70 years of age who were diagnosed with a midshaft clavicle fracture. We excluded five patients who had been previously treated for fracture of the ipsilateral clavicle and one patient who underwent surgical treatment at the time of injury due to other concomitant fractures. The patients were treated conservatively with either an arm sling or a figure-of-eight bandage regardless of any comminution and segmentation of the fracture. These patients were informed that surgical treatments should be considered if the displacement of the fracture increases, if pain persists for more than 6 months from the time of fracture, or if nonunion occurs during the follow-up period. An arm sling or figure-of-eight bandage was used for 6 weeks; tolerable range of motion was allowed, while excessive motion was restricted. Patients were referred to their local primary hospital for regular follow-up. These patients were instructed to re-visit our clinic if a change in treatment plan was needed.
In May 2018, we reviewed the medical records of the 75 eligible patients to investigate their age at the time of injury, sex, dominant arm, side of injury (right or left), injury mechanism, and any other concomitant injuries and medical comorbidities. We reviewed the initial radiographs of all patients and then conducted a telephone survey to evaluate the clinical results at the time of the study.
Radiological Evaluation
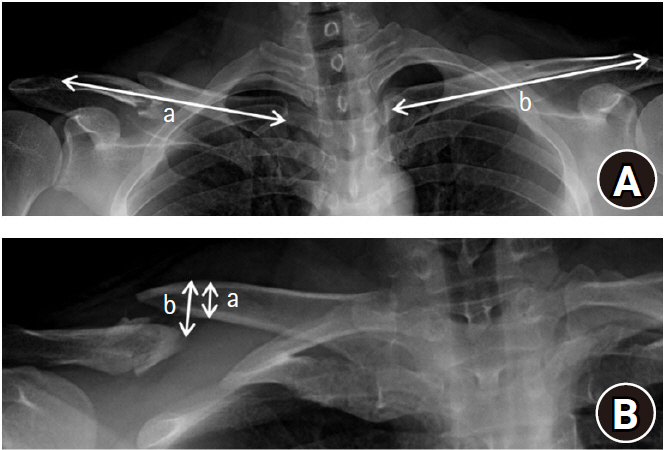
Clavicle fractures were classified according the arbeitsgemeinschaft für osteosynthesefragen (AO) fracture and Dislocation Classification Compendium, which was revised in 2018 [12]. Shortening of the clavicle was defined as the difference between the intact clavicle length and the injured clavicle length as measured on an anteroposterior X-ray. Vertical displacement was assessed by dividing the distance between the superior cortex of both fractured fragments by one bone width of the injured clavicle on a 30° cephalic tilt view X-ray (Fig. 1) [13,14]. Patients were classified according to the presence or absence of cortical contact.
Clinical Survey
In May 2018, 60 of the 75 eligible patients participated in a telephone survey. Patients with pain or other discomfort were encouraged to visit our clinic for further evaluation and counseling. In the telephone survey, the patients were asked whether they eventually received surgery at our hospital or another clinic. For those who underwent surgery, questions about why and when it had taken place were also asked. Patients were also queried about any complications after the surgery and the presence of discomfort or a patient-perceived subjective deformity.
We also verified whether the patient had a confirmation of union from the treating hospital. As part of the clinical assessment, the American Shoulder and Elbow Surgeons (ASES) and pain numeric rating scale (NRS) scores at the time of the telephone survey were also assessed [15]. If the patients complained about pain near the glenohumeral joint area, the degree of pain around the clavicular area was reassessed to differentiate it from other pain due to glenohumeral joint disease. The telephone surveys were performed by a physician who was not involved in treating the patients. Finally, the patients were asked if they would or would not elect to receive surgery again if they were in same situation of clavicle fracture, and the main reason for their answer was recorded.
Statistical Analysis
To analyze the factors associated with the decision to choose surgical treatment, variables including age, sex, involvement of the dominant arm, AO classification, vertical displacement distance, and amount of shortening were included in the univariate analysis (chi-square test for categorical variables and t-test for continuous variables). Variables with a p-value <0.2 upon univariate analysis were included in the multivariable logistic regression analysis. A p-value <0.05 was considered statistically significant.
RESULTS
An analysis of the differences in clinical and radiological parameters between patients who initially received operative treatment and those who received conservative treatment is shown in Table 1. There were no significant differences between the two groups in age, sex, involvement of the dominant arm, injury mechanism, or AO classification (Table 1).
There was no significant difference in the average clavicle shortening distance in patients who received operative treatment (7.8 mm) and in patients who received conservative treatment (3.7 mm, p=0.185). There was also no significant difference in the mean vertical displacement between patients who underwent operative treatment (126.3%) and patients who received conservative treatment (90.9%, p=0.095). Significantly more patients (9/28, 32.1%) with vertical displacement >100% underwent operative treatment than patients (3/32, 9.4%) with vertical displacement <100% (p=0.028) (Table 1).
In the telephone survey, significantly more patients (32/48, 66.7%) reported a subjective deformity after receiving conservative treatment than patients (2/12, 16.7%) who initially underwent operative treatment (p=0.002). There was no significant difference in the number of patients with a confirmed union (P>0.999), ASES score (p=0.784), or a pain NRS score (p=0.795) between participants who underwent operative treatment and those who received conservative treatment (Table 2).
When responding to the question about whether the patient would choose to undergo surgery in the same situation of clavicle fracture in the future, 10 of 48 (20.8%) respondents who initially received conservative treatment answered that they would choose surgery instead. The main reasons for that answer were delayed union or nonunion in four patients, a patient-perceived deformity in five patients, and remaining pain in one patient. More patients (10/12, 83.3%) who had undergone surgery responded that they would choose surgery again if presented with the same situation than patients who received conservative management (10/48, 20.8%; p<0.001). Significantly more patients (13/28, 46.4%) with vertical displacement >100% responded that they would elect for surgery again if in the same situation than patients (7/32, 21.9%) with vertical displacement <100% (p=0.044) (Table 3).
In the analysis of patients who received conservative treatment, five of 19 (26.3%) participants with vertical displacement >100% and five of 29 (17.2%) patients with vertical displacement <100% responded that they would elect for surgery in the same situation again; this result had no significance difference (p=0.449). Significantly fewer patients (7/44, 15.9%) with confirmed union responded that they would elect to have surgery again in the same situation than patients (3/4, 75%) with nonunion (p=0.005). Nine of 32 (28.1%) patients with a patient-perceived deformity and one of 16 (6.25%) without a patient-perceived deformity responded that they would choose surgery if in the same situation, which showed no significant difference (p=0.079).
Variables with p-values <0.2 upon univariate analysis of patient willingness to opt for surgery in the same situation included the following: “previous treatment method” (p<0.001), “vertical displacement” (p=0.044), and “confirmation of union” (p=0.186) (Table 3). A multiple logistic regression analysis was performed using these three variables. “Treatment method” (p=0.001) significantly influenced the decision to undergo an operation in the same future situation, but “vertical displacement” (p=0.246) and “confirmation of union” (p=0.114) were not significantly associated.
DISCUSSION
Patients with midshaft clavicle fracture and a vertical displacement of ≥100% were more likely to eventually undergo surgical treatment than patients with a vertical displacement <100%. Of the 12 patients who had undergone conservative treatment first but eventually received surgery, four chose surgery due to severe pain caused by the fracture. When the vertical displacement is large, any fragments can irritate the skin and periosteum, resulting in greater pain and discomfort [16]. However, due to our small sample size and retrospective study design, we could not analyze the statistical difference in the degree of subjective pain at the initial trauma between the conservative treatment group patients and the operative treatment group patients. Further studies with larger sample sizes that consider this subjective pain as a factor in decision-making will be required.
A substantial number of patients who underwent conservative treatment responded that they would elect for surgery instead if presented with the same situation. This finding likely resulted not only from the presence of nonunions but also patient-perceived deformities or persisting pain until union is achieved, which can result when conservative treatment is chosen as the initial treatment method.
In our study, patients who had undergone surgery had a tendency to respond that they would elect for surgery if faced with the same situation in the future, while patients who had undergone conservative treatment the first time around had a tendency to respond that they would select conservative treatment again. In other words, patients tend to regard the previous treatment method as the correct decision and are likely to select the same method if they experience a similar future injury. However, patients with vertical displacement of ≥100% were significantly more likely to report that they would prefer surgery if they were to experience a similar injury compared to patients who experienced a vertical displacement of <100%.
In the analysis of patients who received conservative treatment, patients with nonunion were significantly more likely to prefer surgery if in the same situation in the future, while patients with a perceived deformity had a tendency (that was not statistically significant) to respond that they would elect for surgery if they ever faced the same situation. This result is in line with previous reports about the consequences of conservative treatment in vertically displaced midshaft clavicle fractures [5,17]. Based on these results, patient-perceived deformity and nonunion of the fracture are likely the most important factors to patients following treatment and affect the satisfaction of patients regarding their fracture treatment method.
Patients with midshaft clavicle fracture with an initial vertical displacement of ≥100% are more likely to eventually undergo surgical treatment due to acute pain, severe deformity, or another doctor’s second opinion. Although there may be no functional deficits, deformity and nonunion may occur in those who choose conservative treatment; therefore, these patients may not be satisfied with their fracture treatment method after some time has passed. This information can be helpful for surgeons and patients when making shared decisions about treatment.
This study had an inherent weakness due to its retrospective study design and small sample size. In addition, the telephone survey did not allow us to confirm the union status of the fracture site with a radiographic examination, and we also could not assess the exact residual deformity of the clavicle (including shortening and angulation) radiographically. Finally, because only the subjective patient-reported outcomes were evaluated by telephone survey, we were unable to conduct an objective evaluation in person and therefore could not objectively assess the long-term outcomes. However, we were able to obtain responses from about 80% of patients, and non-responders did not differ in their demographic characteristics (such as age or sex) from the responders. Because the objective of our study was to determine the factors that influence the treatment strategy selection at the time of trauma, the initial radiographic analysis was sufficient to proceed with our study.
Patients who receive conservative treatment for midshaft clavicle fracture with a vertical displacement of ≥100% may eventually require surgical treatment. If conservative treatment is continued, the patients may be relatively dissatisfied with any residual subjective deformity even though there may be no functional deficit or decrease in union rate compared to patients who initially received surgery.