INTRODUCTION
Numerous methods and scoring systems have been implemented to evaluate and quantify the function in normal and diseased shoulders. The constant shoulder score first published as a university thesis in 1986 is widely accepted among shoulder surgeons and has been mandated by the European Shoulder and Elbow Society [1]. Constant score (CS) incorporates both subjective and objective assessment regardless of the diagnosis, rendering it widely applicable. CS is a 100-point scoring system: 35 points for the subjective assessment (pain, 15 points; arm position and ability to perform daily routine activities, 20 points) and 65 points for the objective assessment (range of motion [ROM]: lateral and forward elevation, internal and external rotation, and shoulder strength) [2].
Shoulder strength and functional demand vary among age groups, sex, and demographic populations [3,4]. The age- and sex-adjusted normative data are essential for any patient-reported outcome measure to ensure the patient outcomes can be compared with similar population cohorts because the normal score values can differ for various populations. Individual-adjusted CS comparing CS of the diseased shoulder with the contralateral side can be used for unilateral shoulder pathologies, however, bilateral shoulder affiliations limit its use. In addition, comparing CS with the contralateral shoulder does not provide the normal CS that should be achieved for a good outcome categorization. The age- and sex-adjusted CSs not only simplify post-injury and post-surgery outcome assessment but also mitigate the biases that may arise due to demographic variation [5].
Normative data for the CS have been published by a few authors representing their respective regional populations (American, Australian, and European) [4,6-9]. Currently, there are no studies in the literature in which South Asian populations, specifically the Indian population, have been investigated. Therefore, in the present study, the age- and sex-adjusted CSs in the normal population were calculated and any gradient of change in the CS with increasing age determined. In addition, the effect of work profile on normal shoulder function was evaluated.
METHODS
The present study included patients who visited the outpatient department for problems other than shoulder (i.e., normal shoulders) and healthy volunteers from the local population. The study was conducted at a tertiary care hospital. Prior to the start of the study, ethical approval from the All India Institute of Medical Sciences, Jodhpur Ethical Committee (No. AIIMS/IEC/2021/3720, Date 06/09/2021) was obtained. Data were collected for more than 3 months after obtaining institutional review board approval. Informed and written consent was obtained from the participants regarding documentation of the research findings. Patients were assured the study results would not affect their treatment protocol.
All the included subjects had normal shoulders according to the original definition given by Constant (no limitation of movements and absence of pain during activities of daily living) [4]. Only patients with no shoulder pain/discomfort when using their shoulder were included in the study. Skeletal maturity was a requirement for inclusion in the study, thus, 18 years was the lower cut-off age. Subjects with any problem that might affect shoulder function (cervical, thoracic spine, rib cage deformity, inflammatory arthritis) were excluded from the study. Any pathology of cervical and thoracic spine or chest might cause painful shoulder movements due to muscle spasm, and inflammatory arthritis can involve the shoulder joint. Therefore, a thorough history was recorded and physical examination performed for each patient to exclude any shoulder pathology. Any specialized test (e.g., magnetic resonance imaging or radiology) was not considered ethical because the participants did not have any symptoms.
Constant scoring of all participants was performed by senior residents under the supervision of the senior faculty. Participants completed questionnaires regarding their subjective pain sensation and ability to perform daily routine activities. ROM was recorded using a goniometer with thoracic spine as reference for abduction. ROM was measured according to recommendations of the European Society for Shoulder and Elbow Surgery [3]. The participant sat in a chair or bed with weight evenly distributed across the ischial tuberosities. During the examination, no rotation of the upper body was permitted and participants had to lift their arm to a pain-free level [3]. To measure the shoulder strength, the recommendations provided by the research and development committee of the European Society for Shoulder and Elbow Surgery in 2008 were followed [3]. A fixed spring balance was used; one end was fixed on the floor and the other end tied with a strap to the wrist of the participant. Subjects were asked to hold the spring balance in >90° abduction in the scapular plane with the palm facing down. The maximum effort at 5 seconds was recorded. Three measurements were taken at 1-minute intervals; the highest reading was used as strength of shoulder abduction [10]. The mean CS was graded according to Bahrs et al. [11] as follows: 86–100, very good; 71–85, good; 56–70, fair; and <56, poor.
All participants in this study were classified based on occupation according to the International Standard Classification of Occupations (ISCO-08) published by the International Labour Organization (ILO) at Geneva in 2012. The ISCO-08 classifies occupational activity into 10 major groups: (1) managers, (2) professionals, (3) technicians and associate professionals, (4) clerical support workers, (5) services and sales workers, (6) skilled agricultural, forestry and fishery workers, (7) craft and related trades workers, (8) plant and machine operators and assemblers, (9) elementary occupations, and (10) armed forces occupations. In the present study, the participants were divided into two categories based on work profile and involvement of physical labor. Category I consisted of the light work group (groups 1–5) and category II consisted of the heavy work group (groups 6–10) [12].
The data collected and recorded on a standardized sheet included demographic variables, relevant history, and the CS with its subsections. For analysis, the participants were classified into six age groups: <20, 20–29, 30–39, 40–49, 50–59, and ≥ 60 years. Descriptive statistics (mean and standard deviation, minimum, maximum, and 95% confidence interval) were calculated for each age group overall and separately for males and females. The mean CS was compared between males and females using the independent t-test. A p-value <0.05 was considered statistically significant. The CS was modeled for each age group using linear regression. A linear standardized equation was estimated for each age group by calculating the adjusted CS for any age belonging to that decade. Statistical analysis was performed using the IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Multivariate regression analysis was performed for various age groups and sex. The independent variables considered were age and occupation. For assessing multicollinearity, collinearity statistics were analyzed using tolerance and variance inflation factor. The tolerance was nearly equal to 1 and variance inflation factor was <v2.
RESULTS
A total of 1,926 patients visited the outpatient department during the data collection period; 1,728 patients were excluded from the study based on the previously mentioned exclusion criteria and 198 patients were finally included in the study. Healthy subjects visiting the hospital as well as patients and hospital staff were selected as controls (n=50). A total of 248 subjects (496 shoulders) were finally enrolled for analysis. The average age of the participants in this study was 37 years and ranged from 18–78 years; 65.7% were males (326 shoulders) and 34.3% were females (170 shoulders) (Table 1). The age and sex distribution of study subjects was not statistically different (p>0.05). Multivariate analysis was performed based on age and occupation as dependent variables. The independent variables were non-colinear.
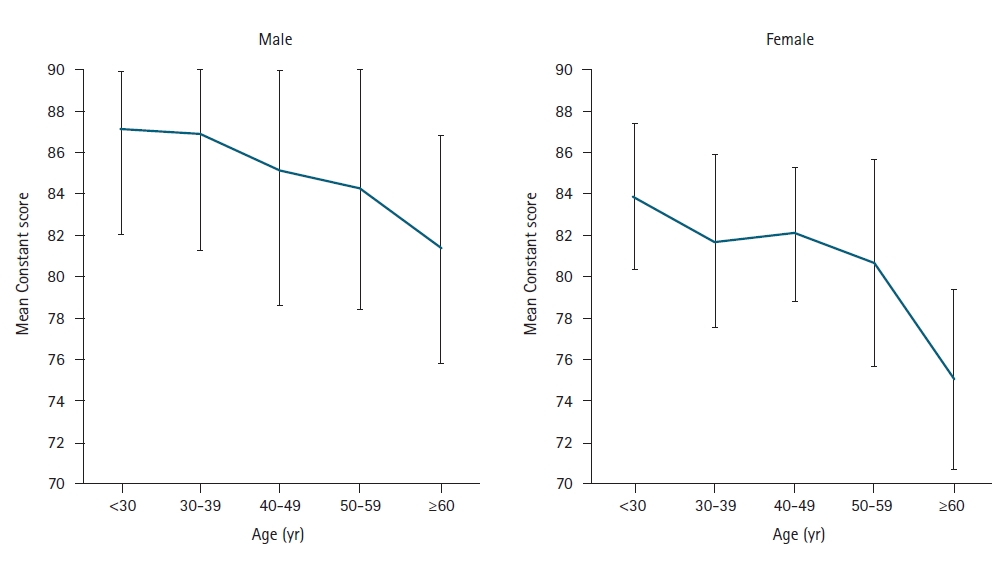
The overall mean CS was 84.6±2.9. The mean CS in males was 86.1±3.0 and 81.8±2.9 in females (p<0.05). The mean CS decreased with age both in males and females and was significant after 50 years of age in males and 40 years of age in females (p<0.05) (Fig. 1). Significant difference was observed between the mean CS for males and females in each age group except the <20 years age group (Table 2). A multivariate linear regression equation was derived based on the present data to calculate the normal adjusted CS at any particular age (Table 3). Among participants, 14% had very good mean CS, 60% good, 25% fair, and 1% poor. The mean CS for the right shoulder was 84.5±3 and 84.8±2.9 for the left shoulder and was not statistically significantly different (p>0.05). Therefore, both shoulders were included for assessment of the overall mean CS (Table 4).
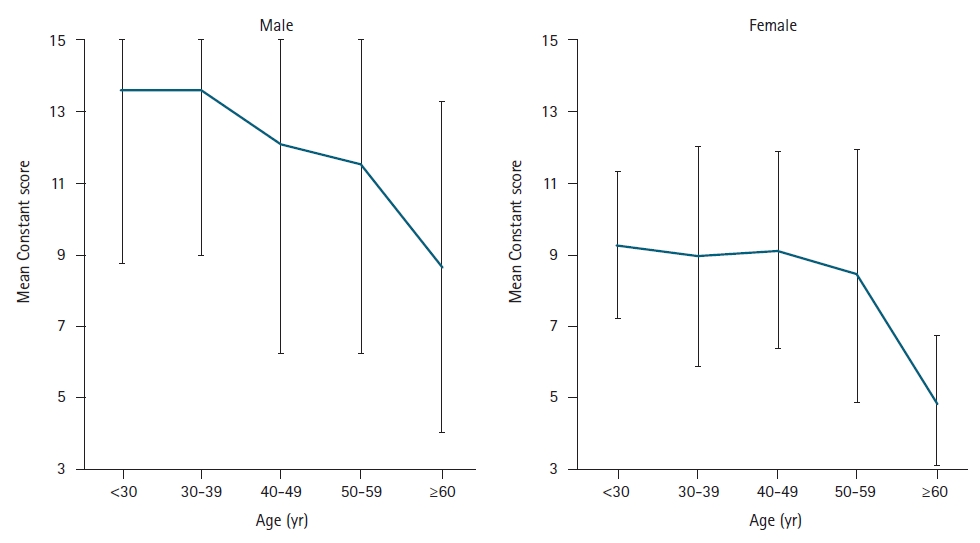
The subjective portion of the CS was equal for all participants because the subjects did not experience pain during shoulder movements, were able to fully perform activities of daily living and/or recreational sports, and sleep was unaffected. All participants were able to move their arm above their head, thus, the subjective score was 35 for all participants. The objective assessment included the strength and ROM measurements. The overall mean strength score was 11.4±2.5. The mean strength score also significantly decreased with age (p<0.05) (Fig. 2). Males had a statistically higher mean strength score (12.9±2.7) than females (8.6±1.6, p<0.05). Forward flexion, lateral elevation, and external rotation did not show any change with advancing age (p>0.05). All participants (except one) scored 10 each in the above three movements. One participant scored 8 points in the forward flexion although she had no functional limitation in her daily activities or job as office clerk. Internal rotation in males remained steady throughout all age decades (CS range, 4–10 points; p>0.05), however, internal rotation in elderly females deteriorated after the fifth decade (CS range, 2–10 points; p<0.05).
In terms of occupational activity, heavy occupational activity subjects (category II) showed a higher mean CS (85.66) than lower occupational activity subjects (category I, 84.29; p<0.05) (Table 5). Although category II patients had higher strength and internal rotation values compared with the category I patients, the difference was statistically non-significant (p>0.05).
DISCUSSION
Method of Measurement
The CS is a reliable outcome measurement method for assessing patients before and after surgical treatment, however, its comparability in patients from different demographic population has not yet been confirmed. Despite the widespread usage and applicability, CS has been criticized due to its poor standardization [13], problems with strength measurement method [14], and inability to evaluate shoulder instability [15]. In 2008, modifications were implemented and a proper methodology with instrumentation was presented, focusing on the assessment method of shoulder abduction strength [3]. Among the multiple methods described by various authors in the literature, the fixed spring balance method and the dynamometer method have been found accurate and reproducible for assessing shoulder strength [16,17]. In the present study, the fixed spring balance method was used. Measuring the strength in the scapular plane provides maximum biomechanical advantage due to the optimum glenohumeral conformity and perfect length-tension ratio in the abductor musculature. This testing position has also been used by Katolik et al. [6] to evaluate the CS.
Age Effect
The functional demands of a young adult male/female differ from an elderly individual. Walton et al. [18] have raised concerns regarding different score results in males versus female patients and score reduction with age. Constant et al. [4] (France) initially observed a steady CS with minimal change across the age groups, followed by a steady decline in males 50 years of age. The variation in scores was higher in females across the age groups. Yian et al. [8] (Switzerland) reported minimal decrease in the CS with aging, especially in females over 40 years of age and males over 60 years of age. Katolik et al. [6] (America) calculated the normalized CS. The authors reported a decrease in CS after 60 years of age, which became significant after 70 years of age in males. The CS decreased in female subjects after 50 years of age. Tavakkolizadeh et al. [7] (UK) reported a decrease in CS in the fifth decade in males, which increased after 70 years of age. The decrease in CS was greater in females after 60 years of age and CS further decreased after 70 years age. The mean CSs in the present study were lower in each age group (Table 6). In the present study, a sharp decrease in CS was observed after 50 years of age in males and 40 years of age in females. The differences in results among studies that included various demographic populations indicates that normative data of the same patient population should be compared. Therefore, normative CS data from different geographic populations are needed.
Sex Effect
In previous studies, statistically significantly higher mean CS was observed in males than in females [4,6-8]. In addition, a similar trend was observed in the present study population with higher mean CSs in males (86.1±3.0) than in females (81.8±2.9, p<0.05). The declining shoulder strength with age and greater shoulder strength in males explain this variation in mean CSs [19,20] allowing reasonable comparisons of outcome scores with age- and sex-adjusted CSs in that population [8]. To compare patients from the same demographic population, an equation based on linear regression for each age group was separately derived in male and female groups. Patient age can be added to the equation to calculate the ideal CS at that age based on the CS in the normal population of the same age group (Table 2).
Score Subsections
The shoulder strength is a major determinant of the CS and contributes 25 points. In the present study, mean strength score significantly decreased with age (p<0.05), and males had a statistically higher mean strength score than females (p<0.05).The strength scores decreased after the fifth decade. Yian et al. [8] also reported statistically higher mean abduction strength in male than in female participants, declining steadily after 40 years of age. In the present study, ROM scores did not change with advancing age in males although females experienced reduced internal rotation after the 5th decade. Significant detrimental effects of aging or sex on shoulder ROM were not proven in previous studies except by Yian et al. [8] who reported decreased ROM with age; however, the change was less than 12°. The lower internal rotation in the elderly female population in the current study could not be explained, however, this could be due to lower functional demand in older females as well as local cultural practices.
Left/Right Side Effects
Significant variations were not found in overall mean CSs between dominant and non-dominant sides as reported in prior studies [4,7,8], which was the reason both shoulders were evaluated in the present study. In addition, the practice of comparing the affected shoulder CS with the opposite shoulder CS can be misleading in shoulder patients because many patients have asymptomatic bilateral shoulder problems which can lead to a false sense of achieving the target CS in postoperative follow-up.
Occupation Effect
Individuals engaged in high-level activities had a higher mean CS than subjects engaged in low-level activities which could be explained because individuals who perform high-level activities have a higher functional demand that requires more muscle strength and shoulder ROM than individuals performing low-level activities. When evaluating the functional outcome of a treatment or surgery using the CS, occupational needs of the patients should also be considered. The normal CS in terms of the job profile of the participants was not assessed in any of the previous studies.
Limitations
The present study had several limitations. The sample size was relatively small. A statistically ideal normative data study requires randomly selected samples from the general population. Another limitation is the non-homogenous data due to the higher number of male participants that could have caused bias. In addition, participants were unequally distributed in the age groups which could create bias in the results. Despite these limitations, the data fairly represents the target population because the participants were from the general population compared with previous studies in which participants were attending a sports medicine clinic [6], resulting in a strong bias because athletes are expected to have better physical activity and shoulder function than the general population. The above-mentioned limitations should be addressed in future studies and the results of this study used as a basis in multicenter research that includes a larger cohort representative of diverse populations.
Conclusion
The results of the present study provide data for the CS in normal shoulders in a specific population and a statistical equation to calculate the expected score at any age. The calculated CS represents the target score to be achieved in a specific age- and sex-matched patient, thus, simplifying the assessment of intervention outcome. The adjusted score derived from our equation allows analysis and comparison of the outcome scores from different hospitals when the standard method of scoring is used. However, differences between the CS data in this study and previously published studies existed, indicating the importance of using normal data from the same population cohort of patients when reporting the outcomes. This is the first study in which normal CS was defined in age- and sex-matched local South Asian subjects without shoulder pathology. Data in the present study regarding age- and sex-adjusted CS can be incorporated in future multicenter studies to better understand and implement the results.