The surgical goal for rotator cuff repair is to restore the anatomical footprint of the rotator cuff tendon with minimal tension and to maximize the contact area and pressure at the tendon to bone interface [1]. Both quantitative (area and height) and qualitative (presence of the fibrocartilage) regeneration of the tendon to bone interface could produce good long-term clinical results by maintaining the structural integrity of the repaired tendon [2,3]. In order to achieve this, sufficient lateral excursion of the torn rotator cuff is a prerequisite. However, surgeons frequently encounter insufficient excursions in many large to massive tears or in some retracted medium tears. A variety of surgical techniques can be utilized to improve tendon excursion, including articular and bursal side release, margin convergence, anterior and posterior interval slide, and medialization of the greater tuberosity. For irreparable tears with non-reducible torn ends, joint sparing salvage procedures including partial repair, repair with various grafts, superior capsular reconstruction, and tendon transfers or shoulder arthroplasty could be performed. Nevertheless, repair of rotator cuff tendons using the remaining tendon, if possible, should yield better results than reconstructive surgery [4].
Supraspinatus advancement was first reported by Debeyre et al. [5] in which the supraspinatus muscles were elevated from the supraspinatus fossa and advanced laterally to obtain sufficient excursion of the torn end. Since then, some surgeons have improved the surgical procedure and reported successful clinical and structural outcomes with supraspinatus advancement [4,6-8]. However, there is no report of all-arthroscopic procedures for supraspinatus advancement without any additional skin incision. Therefore, we present our arthroscopic supraspinatus advancement (ASSA) technique for rotator cuff tears with inadequate excursion. A single orthopedic surgeon (CHJ) performed all procedures.
TECHNIQUES
This study was approved by the Institutional Review Board of SMG-SNU Boramae Medical Center (No. 16-2014-5) and the requirement for informed consent was waived due to retrospective nature of this study.
Patient Positioning and Diagnostic Arthroscopy
All arthroscopic surgeries are performed with patients in the lateral decubitus position under general anesthesia as previously described [9]. Briefly, systematic examination of the glenohumeral joint with standard posterior and anteroinferior portals is followed by that of the subacromial space with lateral and posterolateral portals (Fig. 1A and B).
Glenohumeral Joint Release: Superior Capsulotomy and Coracohumeral Ligament Release
Superior capsulotomy is performed from the 10 to 2 o’clock position (Fig. 1C), and articular-sided coracohumeral ligament release occurs from the base of the coracoid process (Fig. 1D). Superior or three-sided release for the subscapularis tendon is performed if necessary. Care is taken not to involve instrumentation more than 2 cm medial to the superior glenoid margin, especially in the 10 or 2 o’clock position to avoid injury of the suprascapular nerve.
Subacromial Space Release: Superior Release and Coracohumeral Ligament Release in Continuity
Bursal tissues and adhesions overlying the supraspinatus or infraspinatus and those around the coracoid process and scapular spine are removed (Fig. 1E). Identification and release of the suprascapular artery and nerve around the suprascapular notch are performed if necessary. After release, lateral excursion of the torn end is re-evaluated to determine the need for ASSA.
Anterior Compartment Elevation of the Supraspinatus in the Supraspinatus Fossa
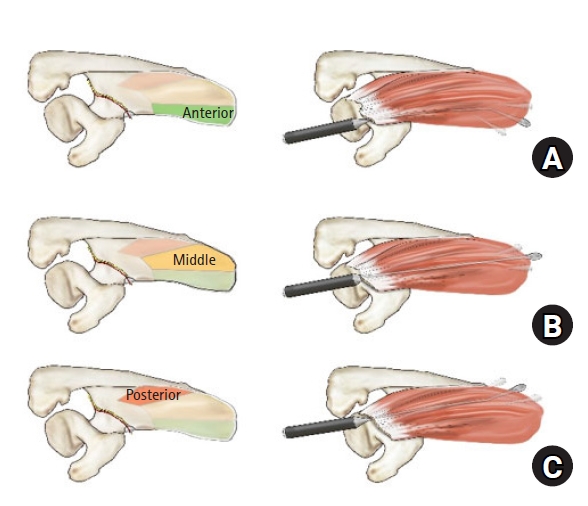
Three sutures are threaded into the torn end for traction. The insertion anatomy of the supraspinatus muscle consists of larger anterior (A) and smaller posterior parts (P), each of which is further subdivided into superficial (S), middle (M), and deep parts (D) [10]. For meticulous elevation of each muscle origin, we developed the three-compartment elevation procedure with anterior, middle, and posterior sections. For anterior compartment elevation, the traction sutures are pulled out through the posterior portal to secure clear vision around the base of the coracoid process and the suprascapular notch. Using the base of the coracoid process as a jig (Fig. 2A), a specially modified, long, narrow, and right-curved Cobb elevator for the right shoulder is inserted through the lateral portal and placed at the entrance of the supraspinatus fossa located just medial to the supraspinatus notch (Fig. 1F).
The Cobb elevator is then slid medially along the fossa to elevate the anterior portion of the AM attached to the medial two-thirds and the AD attached to the lateral one-third of the supraspinous fossa and along the anteromedial border of the fossa for elevation of AS. The Cobb elevator must be moved slowly and carefully around the suprascapular notch so as not to injure the suprascapular nerve. Using the surgeon’s other hand, one can estimate the location of the Cobb elevator tip along the medial border of the scapula. Complete elevation from the fossa is required to achieve larger excursions, especially from the medial border of the scapula.
Middle Compartment Elevation of the Supraspinatus in the Supraspinatus Fossa
The traction sutures are pulled out through the accessory lateral portal just lateral to the acromion. A modified, long, narrow, downward curved Cobb elevator is introduced through the lateral portal and passed between the torn tendon and superior labrum. Using the superior glenoid margin as a jig (Fig. 2B), it is placed on the entrance of the supraspinatus fossa (Fig. 1G). The Cobb elevator is then slid medially along the entire supraspinatus fossa to elevate the middle portion of the AM attached to the medial two-thirds, the AD attached to the lateral one-third, and the PD attached to the base of the supraspinatus fossa.
Posterior Compartment Elevation of the Supraspinatus in the Supraspinatus Fossa
A modified, long, narrow, left-curved Cobb elevator for the right shoulder is introduced through the lateral portal between the tendon and the labrum but more posteriorly directed compared to middle elevation (Fig. 2C). Posterior compartment elevation involves the posterior portion of the AS that is attached to the medial one-third of the superior border of the scapular spine, as well as the PS and PM that are both attached to the posterior wall of the supraspinatus (Fig. 1H). Lateral excursion is verified after each elevation procedure and repeated as needed. A lateral excursion of approximately 4 to 5 cm should be obtained using the three-compartment elevation procedure.
Postoperative Protocol and Exercises
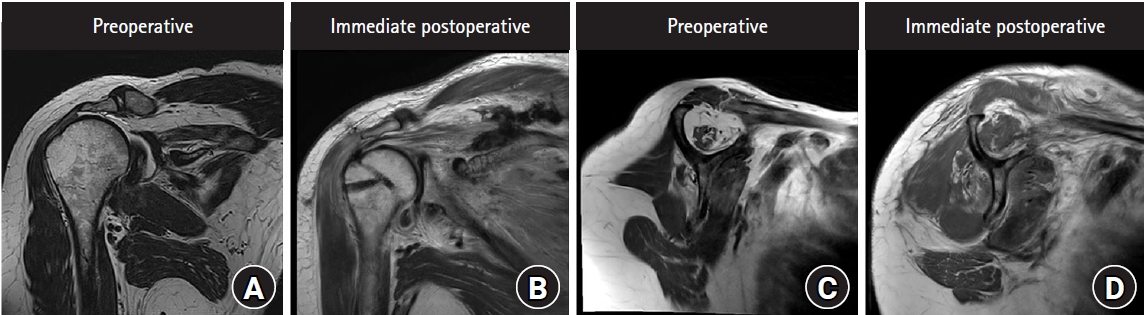
The patients are instructed to undergo postoperative magnetic resonance imaging within 3 days following surgery (Fig. 3). The shoulder is immobilized for 6 weeks using an abduction brace. Shrugging, protraction, and retraction of the shoulder girdles; intermittent exercises of the elbow, wrist, and hand; and external rotation of the arm to neutral with the brace are encouraged as tolerated, typically starting immediately after surgery. Further passive range of motion (ROM) and active assisted ROM exercises are allowed after the patient is gradually weaned off the abduction brace 6 weeks after surgery. Patients begin strengthening exercises after 3 months. Light sports activities, such as jogging, are allowed after 3 months, and a full return to sports is allowed after 6 to 9 months based on individual recovery.
DISCUSSION
Debeyre et al. [5] first proposed that the supraspinatus can be advanced laterally by elevating the entire muscle from its fossa. However, this procedure required a large skin incision, acromion osteotomy, and a deltoid split, all of which may result in significant complications. The surgical procedure has been modified to avoid acromion osteotomy [12], to maintain the deep fasciae between the levator scapulae and the supraspinatus and between the rhomboids and the infraspinatus [6], and to convert the procedure from open to arthroscopic-assisted surgery with 4 cm [7] and 2 cm incisions around the medial scapular spine [8]. However, all of these surgeries require an additional skin incision or portal around the medial scapular border, with need for wider and fastidious skin preparation. Furthermore, with a small 2 cm portal, it would be difficult to pass through the trapezius without additional damage to this thin muscle and to precisely locate the supraspinatus and infraspinatus for elevation. Therefore, we introduce ASSA as the first all-arthroscopic procedure for rotator cuff muscle advancement. Using modified, long, narrow, curved Cobb elevators, all of the muscle elevation procedures can be performed through lateral portals without any additional incisions. Through the stepwise three-compartment elevation procedure based on supraspinatus anatomy, surgeons could safely elevate the supraspinatus muscle from the fossa and sufficiently advance it laterally as necessary. With ASSA, we consistently gained 4 to 5 cm of additional lateral excursion. We believe that ASSA could ensure maximal restoration of the anatomical footprint of the rotator cuff tendon while maintaining minimal tension to optimize the healing process and result in robust structural integrity. In addition, arthroscopic infraspinatus advancement (AISA) or arthroscopic subscapularis advancement (ASCA) can also be achieved using the surgical procedures and instruments used in ASSA. Nevertheless, AISA is performed when further advancement of the infraspinatus is required. During the AISA procedure, the lateral portal serves as the viewing portal, while the Cobb elevator is inserted through the posterolateral portal. An additional accessory portal can be created posterior to the posterolateral portal in order to accommodate the Cobb elevator. Using the scapular spine as a reference for dividing the supraspinatus and infraspinatus muscle bellies, the Cobb elevator is advanced under the infraspinatus muscle to create detachment from the bone. During the ASCA procedure, the lateral portal serves as the viewing portal, while the Cobb elevator is inserted through the additional anterosuperolateral portal. The Cobb elevator is advanced under the subscapularis muscle to create detachment from the bone.
Originally, supraspinatus muscle advancement included fascial detachment from the medial scapular border and spine [5,12]. Later, Kurokawa and Hirasawa [6] introduced a modified procedure that maintained the fascial connection between the rotator cuff muscles and the rhomboids. Currently, some surgeons retain the fascial connection [7], while some other surgeons do not [4]. However, the clinical importance of maintenance of the fascial connection remains unclear as both groups report satisfactory clinical and structural outcomes. Practically, it would be difficult to maintain the fascial connection as elevators are only introduced through lateral portals, and the tense fascial connection due to arm traction would be more prone to splitting than detachment from the medial border of the scapula. Meanwhile, lateral excursion will increase in the absence of any soft tissue restraints to the supraspinatus muscle. In our experience, division of the fascial connection and complete elevation of the supraspinatus increased lateral excursion by at least an additional 1 or 2 cm. Therefore, dividing fascial connections and completely elevating the supraspinatus in ASSA would be viable options in some cases.
As opposed to open supraspinatus muscle advancement that was performed without suprascapular nerve release [5,12], most arthroscopic-assisted surgeries were reported to be performed with release [4,7,8]. Several studies described concerns of suprascapular nerve injury in massive rotator cuff tears [13] and in repair surgeries with large lateral advancements [14]. However, there have been no reported cases of suprascapular nerve injuries in supraspinatus muscle advancements with or without nerve release. In our experiences with ASSA, we also have not experienced nerve injury regardless of release. Therefore, we do not believe that suprascapular nerve release is obligatory for ASSA.
Repairs are always preferable to reconstruction or replacement when possible since the former is more anatomic, biologic, and enduring [4]. In that sense, we suggest ASSA as a useful surgical technique for managing challenging retracted rotator cuff tears with inadequate lateral excursion to aim to convert irreparable tears to reparable tears in selected patients.