INTRODUCTION
Prosthetic shoulder arthroplasty (PSA) provides excellent pain relief and restores function in patients with glenohumeral arthritis. PSA performance has increased significantly [1-4] because of greater patient expectations, proven clinical outcomes, and implant durability. Specifically, anatomic total shoulder arthroplasty (TSA) is preferred over hemiarthroplasty (HA), at least for patients with primary glenohumeral osteoarthritis, because of documented superior outcomes and durability [5,6].
In addition, the indications for PSA have expanded to new patient populations, including increasingly younger patients with specific types of glenohumeral arthritis, such as post-traumatic arthritis, chondrolysis, and capsulorrhaphy arthropathy. Particularly, post-arthroscopic chondrolysis is a rare but devastating condition characterized by rapid cartilage destruction with associated high pain level and stiffness. Chondrolysis has affected patients as young as 15 years [7] and has been associated with prominent suture anchors, excessive use of heat, and intra-articular infusion of local anesthetics [8].
Despite the benefits of PSA, concerns over long-term durability have limited its use in young patients [9]. These concerns have motivated the development of non-prosthetic alternatives, including arthroscopic and open reparative and biologic interventions. Specifically, osteoarticular autograft transfer or allograft surgery [10-12], as well as arthroscopic procedures including debridement, resection of osteophytes, microfracture, and capsular release, coupled with adjunctive procedures such as biceps tenodesis and subacromial decompression are being performed in young patients with glenohumeral arthritis [10,12-17]. Some have advocated arthroscopic intervention even for advanced disease [14,15], but long-term effectiveness remains unknown, and both short-term effectiveness and reproducibility have been questioned, especially in patients with bipolar joint disease [10,13,17,18]. Furthermore, some types of glenohumeral arthritis, such as chondrolysis, are refractory to nonoperative and arthroscopic interventions and frequently require PSA [19,20].
The precise definition of “young” patient, as pertaining to PSA, is also evolving. Most previous reports adopted thresholds of 50 or 55 years of age to characterize patients as young [9,21-26]. However, much younger patients also undergo PSA [19,20,27]. The generalizability of published results of PSA in patients approaching 50 years of age is unproven. Understanding the outcomes of PSA in young patients is important for several reasons. Young patients often have the highest expectations and greatest demands for both work and sport. Second, their life expectancy is longer, increasing the importance of identification of risk factors for early failure or revision. Third, the number of patients undergoing PSA, including young patients, is projected to continue to increase [3].
To our knowledge, there are no published data on the outcome of PSA in a cohort composed entirely of patients who are much younger than 50 years. The purpose of this study is to report on outcomes following PSA, stratified by surgery and by diagnosis, in patients who are 40 years or younger. There are several studies looking at patients younger than 50 including articles by Sperling et al. [24-26]. Our hypothesis is that TSA provides better clinical outcomes and implant durability compared with HA, including resurfacing hemiarthroplasty (RHA). Our secondary hypothesis is that patients with chondrolysis have inferior outcomes following PSA than do those with other diagnoses.
METHODS
This study was conducted in compliance with Good Clinical Practices. Data included in this study were prospectively collected as part of the senior author’s standard of care. Internal review by our ethics committee was completed, but formal Institutional Review Board approval was not required. Informed consent was not required for this retrospective study because all data recorded, analyzed, and reported were obtained routinely as part of the senior author's clinical practice.
All primary PSAs performed by the senior author between January 2008 and December 2017 in patients 40 years and younger were identified. As stated, younger than 40 years excludes patients who are 40 years old, but we included these patients. The type and number of previous surgeries and underlying diagnoses were recorded for each patient. Surgeries were stratified as either RHA or TSA. The results from two patients undergoing stemmed HA with concentric glenoid reaming, often referred to as the ream-and-run procedure, were included in the TSA group. This classification was used because of the similar peri-glenoid soft tissue releases and glenoid surface preparation (other than glenoid component insertion) as well as indication of glenohumeral arthrosis with more severe glenoid wear. This differentiated these cases from RHAs, which were performed in patients with concentric and generally milder glenoid wear. All patients underwent preoperative standardized bi-planar radiographs and either magnetic resonance imaging or computed tomography scan.
All PSAs were performed through a deltopectoral interval with subscapularis peel. Anterior and inferior capsular release was carried out in all patients, but the labrum was preserved unless a glenoid implant was being inserted. Except in a few of the youngest patients treated early in the study period, the biceps tendon was tenodesed routinely. All humeral implants were inserted without cement, and all glenoid implants were composed of all-polyethylene cemented components. Subscapularis repair was performed using transosseous sutures for TSA and three to four double- or triple-loaded suture anchors for RHA. No patient 40 years or younger underwent reverse shoulder arthroplasty, stemless TSA, or glenoid resurfacing using a tissue patch during the study period.
Patients underwent standardized measurement of active range of motion including forward elevation, abduction, and external rotation at the side, all of which were expressed in degrees; and internal rotation to the back, expressed as the highest spinous process level attained with the thumb on the operative side. Internal rotation levels were transformed to a 10-point scale as for the Constant score [28]. Self-assessed outcomes were evaluated pre-operatively and at the most recent follow-up using the 10-point visual analog scale (VAS) for pain, the Simple Shoulder Test (SST), and the American Shoulder and Elbow Surgeons (ASES) score. True AP in external rotation (Grashey) and axillary-lateral plain radiograph views were obtained in all but two patients at most recent follow-up. In addition, intraoperative and postoperative complications and all repeat operations, including revision shoulder arthroplasty, were identified and reported.
Statistical Analysis
Preoperative active range of motion, SST, ASES, and VAS pain scores were compared to those at the most recent follow-up. Final range of motion and self-assessed outcome, as well as improvements in both, were also compared between RHA and TSA. Similarly, the results for chondrolysis were pooled and compared to those for the other diagnoses. Statistical analysis was performed on Excel (Microsoft Excel for Mac, Redmond, WA, USA) using the paired or unpaired t-test or Wilcoxon signed rank test, as appropriate.
RESULTS
Between January 2008 and December 2017, the senior author performed 1057 PSAs, including 511 anatomic TSAs, 400 reverse TSAs, 94 stemmed HAs, and 52 RHAs, including revisions. Forty-two of these (4.1%) were performed in patients 40 years or younger. Five patients younger than 40 years underwent revision shoulder arthroplasty, including two patients in this study, but their outcomes following revision shoulder arthroplasty are not included. Two additional patients were excluded because PSA was performed as part of salvage revision surgery for recurrent traumatic anterior shoulder instability with combined massive glenoid and humeral bone loss, and five patients (six shoulders) were lost to follow-up. The remaining 29 shoulders in 26 patients were available for clinical and self-assessment follow-up at a mean of 5.0 years (range, 24 months–11 years) postoperatively.
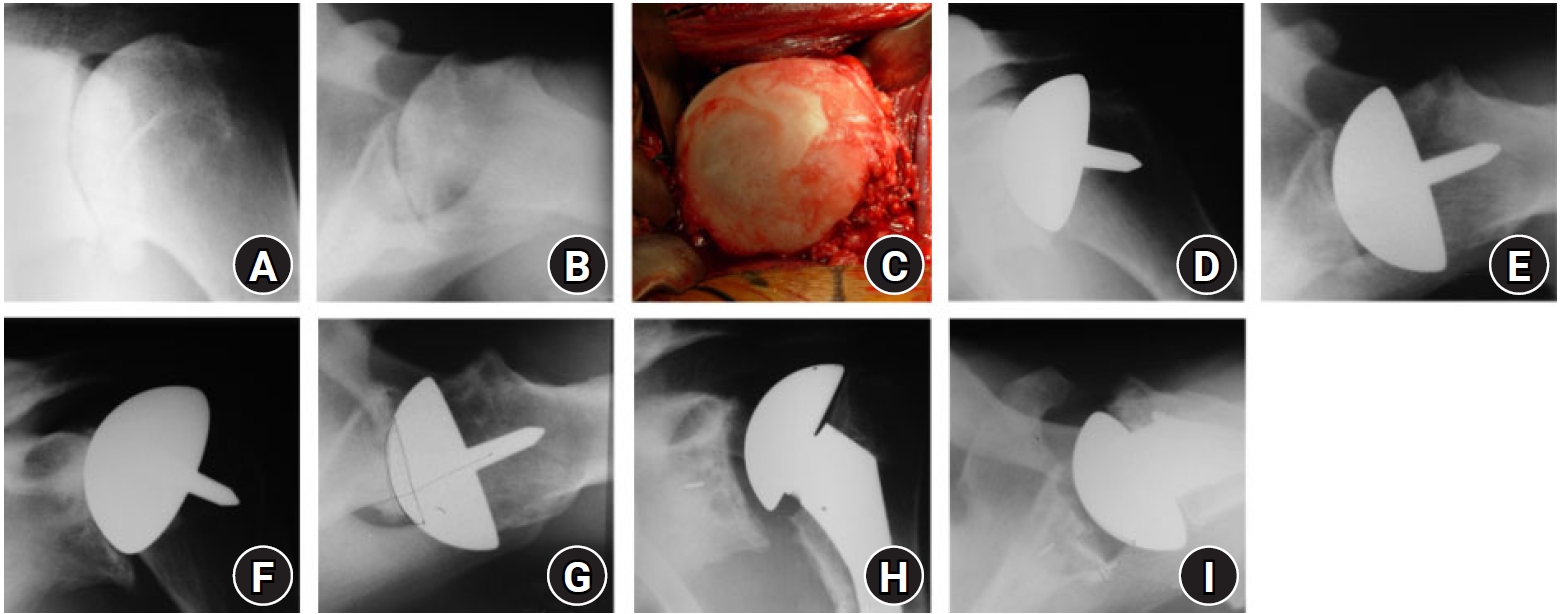
Nine shoulders in eight patients underwent TSA, including three shoulders in two patients undergoing the ream-and-run procedure. Twenty shoulders in 18 patients underwent RHA (Figs. 1 and 2). Twelve shoulders underwent PSA for chondrolysis, seven shoulders for osteonecrosis, six for capsulorrhaphy arthropathy, two for primary osteoarthritis, and two for post-traumatic arthritis. Twenty-one of 29 shoulders (72.4%) underwent previous surgery (range, 1–3 surgeries), including 21 of 22 shoulders with a diagnosis other than osteonecrosis. Patient characteristics, including type of PSA, are shown in Table 1, stratified by diagnosis. Follow-up for PSA performed for chondrolysis was significantly longer than that for PSA performed for other diagnoses (7.2±2.6 years vs. 3.7±2.2 years, p<0.001).
Nineteen PSAs were performed in 17 male patients and nine PSAs in nine female patients. Mean age at arthroplasty was 31.2 years (range, 17–40 years). With the numbers available, patients undergoing primary PSA for chondrolysis were significantly younger than patients undergoing PSA for other diagnoses (25.6 vs. 35.1, p<0.001). Additionally, patients undergoing RHA were slightly younger (30.2 vs. 33.3 years, p=not significant) than those undergoing TSA.
For the entire cohort at the most recent follow-up, mean active forward elevation improved from 102° preoperatively to 141°, active abduction improved from 91° to 126°, active external rotation improved from 26° to 43° (p<0.001 for all), and active internal rotation improved from L5 to T12 spinous process (p<0.005). Mean VAS-pain score improved from 6.3 to 2.1 (p<0.001), mean SST improved from 4.0 to 9.0 (p<0.001), and mean ASES score improved from 38 to 75 (p<0.001).
The outcomes stratified by diagnosis and by treatment are demonstrated in Tables 2 and 3, respectfully. Patients undergoing TSA had less preoperative external rotation than patients undergoing RHA (14° vs. 31°, p<0.05). Otherwise, RHA and TSA patients had similar pre- and postoperative range of motion and outcomes scores. Patients undergoing PSA for chondrolysis as well as those receiving PSA for other diagnoses had similar pre- and postoperative range of motion and outcomes scores (p>0.05).
There were no intraoperative or immediate postoperative complications. Seven of 29 shoulders (24.1%) have undergone 11 reoperations, including five revision shoulder arthroplasties. Three RHAs underwent revision to TSA, including a revision performed elsewhere for progressive glenoid erosion at 8 years postoperatively. One patient underwent two-stage revision to reverse shoulder arthroplasty for glenoid implant loosening with uncontained glenoid defect requiring structural bone graft at age 47 years, 8 years postoperatively. One ream-and-run patient underwent single-stage reimplantation for prosthetic joint infection. Four of five shoulders undergoing revision surgery had an original diagnosis of chondrolysis.
Additionally, the ream-and-run patient underwent arthroscopic lysis of adhesions twice, before and after single-stage revision. The patient who was ultimately revised from RHA to TSA at 8 years postoperatively had previously undergone arthroscopic lysis of adhesions 18 months after RHA. One patient underwent arthroscopy-assisted open biceps tenodesis 3 months postoperatively, with a good clinical result maintained at 8 years postoperatively. Finally, one patient who underwent bilateral ream-and-run procedures underwent left suprascapular nerve release elsewhere, with substantial improvement in symptoms and good clinical result maintained at 4 years postoperatively.
DISCUSSION
PSA for glenohumeral arthritis in young patients is a challenging proposition because patients often expect, in addition to pain relief, the ability to return to physical work or sports [21,23]. For some patients, these expectations remain unmet after PSA; for others, return to strenuous activities places greater motion and loading demands on the PSA and might lead to accelerated wear or early loosening. Additionally, the underlying diagnosis in young patients is typically inflammatory arthritis or various types of secondary arthritis such as chondrolysis, capsulorrhaphy arthropathy, or osteonecrosis, rather than primary osteoarthritis. Therefore, these patients present with a unique set of complex pathologies and treatment challenges [29].
Not surprisingly, patient satisfaction in younger patients following PSA has historically been disappointing. Schoch et al.[24] and Sperling et al. [25,26] have reported on the results of HA and TSA in patients with glenohumeral arthritis who were younger than 50 years. Follow-up at 15 years confirmed long-term pain relief and improvement in shoulder motion after both procedures. Still, 60% of patients undergoing HA and 48% of patients undergoing TSA were dissatisfied with their result [26]. More recently, Wagner et al. [30] studied the role of age in the outcomes and complications of PSA in a large institutional database and found that the risk of revision surgery decreased linearly between ages 40 and 85, with each 1 year increase in age showing a 3% decrease in risk of revision. The authors [30] concluded that there is a strong association between young age and increased rates of revision surgery and reoperation because of mechanical failure after PSA.
Our study included patients undergoing RHA and TSA. In general, RHA was performed on patients younger than 30 years or when the glenoid was unaffected or concentrically eroded; otherwise, TSA was performed. An economic decision study employing a Markov chain decision tree model demonstrated an advantage of TSA over HA in patients between age 30 and 50 years [31]. Compared with HA, TSA required fewer revisions, greater cost savings, and greater quality adjusted life years gained. HA avoids the problems associated with glenoid implantation, including late loosening. However, painful glenoid erosion may hasten the need for revision surgery.
RHA aims to avoid humeral head resection and use of an intramedullary stem and to preserve the native anatomy of the glenohumeral joint. Optimal positioning of the resurfacing implant should, in theory, preserve native humeral head inclination, offset, and version and facilitate late revision to an anatomic TSA when this becomes necessary [32]. Levy et al. [33] reported 81.6% survivorship and high patient satisfaction at a minimum of 10 years following RHA in a group of patients aged 50 years or younger, with a mean age of 39 years. Other studies have demonstrated good short- and mid-term clinical results and durability in younger patients [21,34-36], although at least one study has demonstrated poor durability and patient satisfaction [37].
Survivorship of TSA has typically exceeded that of HA. Schoch et al. [24] reported that survivorship of HA was 82% at 10 years and 75% at 20 years; and survivorship of TSA was 97% and 84% at 10 and 20 years, respectively . However, most of the patients in that study had post-traumatic or inflammatory arthritis, and none had chondrolysis [24,26]. In a related study employing the same institutional database, Bartelt et al. [22] studied the long-term outcomes of PSA specifically for osteoarthritis in patients younger than 55 years. Implant survivorship at 10 years was 92% for TSAs and 72% for HAs [22]. Substantial glenoid periprosthetic lucencies or a shift in component position was identified in 10 of 34 TSAs, and at least moderate severity glenoid erosion was identified in 6 of 13 HAs. However, the authors concluded that TSA offered advantages over HA in terms of pain relief, shoulder range of motion, and implant survival [22]. Eichinger et al. [23] evaluated patient satisfaction and implant durability rates following PSA. The authors reported 5-year survivorship of 89% for HA and 95% for TSA. However, corresponding rates of patient satisfaction at 5 years were 72% and 95%, respectively. The authors noted discordance between patient satisfaction and implant survival, especially for HA [23].
In the youngest and most active patients, the benefits of a polyethylene glenoid implant may need to be balanced against the risk of glenoid implant loosening. Concerns over glenoid implant loosening and progressive glenoid erosion have motivated the development of alternatives including biologic glenoid resurfacing and the ream-and-run procedure [12,38]. No patient in this series underwent biologic glenoid resurfacing using soft tissue interposition because of a preponderance of studies demonstrating poor outcomes and survivorship when using this procedure [39-43]. For example, Elhassan et al. [39] reported that 10 of 13 patients (77%) undergoing HA combined with biologic glenoid resurfacing required revision to TSA for persistent pain at a mean of 14 months follow-up. Radiographs demonstrated rapid and progressive joint space narrowing and glenoid erosion. Muh et al. [44] demonstrated initial improvements in pain and function following HA with biologic glenoid resurfacing in patients 55 years old or younger, but the revision rate was 44% at a mean 36 months follow-up. A recent systematic review of the results of biologic glenoid resurfacing combined with HA documented an overall complication rate of 36%, a revision surgery rate of 34%, and a clinical failure rate of 43% [45].
The ream-and-run procedure combines HA with concentric spherical glenoid reaming to correct glenoid articular surface incongruity in order to recenter the humeral head and create durable glenoid articulation without implant or graft [46-53]. The procedure provides an alternative to TSA using a conventional all-polyethylene glenoid implant. Its development was motivated by concerns over early glenoid implant loosening, especially in younger, more active patients, and the unpredictable results following either glenoid implant removal or revision implantation [49]. Recent studies have demonstrated higher rates of return to sports and strenuous work following ream-and-run compared with TSA [48,52]. In our series, one patient with severe bilateral posterior glenoid erosion and dysplasia underwent staged bilateral ream-and-run procedures at 20 and 24 years of age to partially correct glenoid version and create a smooth articulation. Another patient with capsulorrhaphy arthropathy underwent ream-and-run at age 32 years.
The mean age of patients undergoing PSA in this series was only 31.2 years, which is nearly a decade younger than in any previously published report. Additionally, the mean age of patients undergoing RHA was only 30.2 years; and RHA was performed in 8 of 10 shoulders performed at age 26 years or younger. We did not consider implanting a glenoid component in these patients for several reasons: to preserve glenoid bone stock for eventual revision, to avoid the glenoid exposure challenges that accompany humeral head preservation, and to avoid the risk of early glenoid implant failure.
Three of 20 RHA patients (15%) required revision to TSA, at 30, 42, and 91 months postoperatively. All three patients had chondrolysis and developed progressive glenoid erosion, and none had evidence of implant loosening or any intraoperative or postoperative signs of prosthetic joint infection. All three patients reported improvements in range of motion and outcome following their revisions.
Six all-polyethylene glenoid components were implanted in this series of patients 40 years or younger, comprising the nine in the TSA group less the three ream-and-run procedures. One patient underwent staged glenoid implant removal and bone graft of an uncontained glenoid defect at age 47 years and 95 months postoperatively, followed by revision to reverse shoulder arthroplasty 3 months later. The remaining five glenoid components have survived for a mean follow-up of 78 months.
The rate of revision surgery varied by underlying diagnosis. Twelve patients in this series were initially diagnosed with chondrolysis, accounting for nine of the 10 shoulders. The patients undergoing PSA were 26 years or younger. Four of the five PSAs that underwent revision, including that performed at a different care facility, were patients with chondrolysis. This includes three RHA patients who underwent early revision for glenoid arthrosis and a single TSA patient who underwent revision for glenoid loosening at approximately 8 years postoperatively. Overall, four of 12 (33.3%) shoulders with chondrolysis have undergone revision PSA, compared to only one shoulder with another diagnosis.
Chondrolysis patients demonstrated high revision rates, which may relate to the underlying diagnosis as well as the development of painful glenoid arthrosis following RHA. However, these high rates may also relate to their young age and substantially longer duration of follow-up than patients undergoing PSA for other diagnoses (7.2 vs. 3.7 years). In a large retrospective review of a single health care system database, Dillon et al. [54] reported that patients younger than 59 years had a two-fold higher risk of early revision than patients older than 59 years following PSA. A recent multicenter study evaluating the results of treatment for osteoarthritis and capsulorrhaphy arthropathy in patients 50 years or younger found that complication and revision rates were substantially higher following HA than TSA [55]. Another study recently demonstrated that prior non-arthroplasty surgery was associated with inferior patient reported outcomes and higher revision rates after TSA [56]. Collectively, these studies raise concerns over the influence of diagnosis, prior surgeries, and high functional demands experienced by young patients on implant durability and the need for revision surgery.
Several studies have noted the relatively modest functional gains and high pain levels following PSA for chondrolysis [19,20,27]. We previously reported on the short-term results of PSA for glenohumeral chondrolysis that included patients older than age 40 and found that mean active forward elevation improved 47° to 140°, mean active abduction improved 50° to 131°, and mean active external rotation improved 27° to 49°; these were all statistically significant improvements [19]. In addition, mean VAS-pain scores improved significantly to 3.4; and mean ASES scores and SST improved significantly, from 37 to 66 and from 4 to 8, respectively.
Levy et al. [27] reported on 11 patients with a mean age of 39, ranging from 16 to 64 years and including two patients, aged 16 and 18 years, who underwent total shoulder replacement for chondrolysis. The authors [27] found statistically significant improvements in range of motion, including gains of 34° in active abduction and 22° in active external rotation; but the 16° improvement in active forward elevation was not statistically significant due to limited sample size. In addition, ASES scores improved significantly from 30 to 77 and SST from 3 to 8 [27]. The ASES pain score improved to 36.4, equivalent to a VAS-pain score of 2.9.
Schoch et al. [20] reported on 26 patients undergoing PSA for chondrolysis after shoulder arthroscopy including patients 21 to 58 years old with a mean age of 40 years. Twenty-three of 26 patients were followed for a minimum of 2 years or until reoperation, with a mean follow-up of 4 years, comparable to the follow-up in the present series. The authors [20] found that pain scores improved from 4.7 to 2.6, but only 14 of 23 patients decreased to mild or no pain. Five of 23 patients (21.7%) required reoperation, including two for glenoid loosening and one each for infection, instability, and stiffness [20]. Mean ASES score was 64, and eight patients (35%) rated their shoulder as the same or worse [20]. The authors concluded that, although PSA for chondrolysis improves pain and mobility, patient satisfaction is variable, and the reoperation rate is unexpectedly high. Therefore, patients undergoing PSA for chondrolysis should be counseled about postoperative expectations [20].
Collectively, the results of previous studies and those presented here indicate challenges in treating relatively young patients with end-stage glenohumeral arthritis. These patients often have residual shoulder pain following PSA, which dampens their self-assessed outcomes. This is especially true of patients with chondrolysis, who often present with high pain levels and marked joint stiffness and who respond less predictably to PSA. In addition, although avoidance of a glenoid implant may be desirable, the rate of revision from RHA to TSA reported here is concerning, especially given the young patient ages. No fewer than five of the 29 shoulders in this series have undergone multiple subscapularis tenotomy for surgical exposure during PSA, causing concerns over the potential for subscapularis muscle atrophy and tendon attenuation and a negative clinical impact over time.
Study limitations include a relatively short follow-up of a small cohort of patients with heterogeneous diagnoses and treatments. However, the varied diagnoses underscore the reality that young patients today develop end-stage glenohumeral arthrosis, rather than primary osteoarthritis or inflammatory arthritis, from prior surgery or other treatments. Longer follow-up will be needed to evaluate the overall survival of both RHA and TSA cohorts. However, this study represents an initial report on the outcomes of relatively young patients following PSA.
This study demonstrates that PSA in young patients provides substantial improvement in active range of motion and patient reported outcomes in most patients, irrespective of diagnosis and glenoid management. However, one-third of chondrolysis patients underwent revision surgery during the study period, including three RHAs revised to TSAs due to glenoid wear. Therefore, we cannot recommend RHA in chondrolysis cases. Additionally, RHA should be considered with caution in young patients and performed only after shared decision-making and counsel about the risk of early revision to TSA.