Arthroscopic repair of large and massive rotator cuff tears—“sandwich augmentation” with the long head of the biceps tendon: a technical note
Article information

Abstract
For most shoulder surgeons, addressing massive rotator cuff tears that have retracted ends poses a significant challenge. This study introduces a technique, termed the “sandwich augmentation technique,” which incorporates the long head of the biceps tendon (LHBT) into a single-row rotator cuff repair. The procedure, performed arthroscopically with the patient in the lateral decubitus position, involves attaching the LHBT and rotator cuff tissues together to the greater tuberosity. This effectively sandwiches them within the rotator cuff footprint. The goal of this technique is to enhance the thickness of the fully interposed cuff margin, thereby providing better support for the repair. The sandwich augmentation technique, which integrates the biceps into the rotator cuff repair, has demonstrated positive clinical outcomes and moderate anatomical results. It also prevents superior migration of the humeral head in cases of large or massive rotator cuff tears. Further research is required to assess the long-term effectiveness of this procedure.
Arthroscopic and open surgical techniques for repairing rotator cuff tears have shown varying degrees of success. Arthroscopic repair can effectively treat small- to medium-sized tears, but large or massive tears pose significant challenges due to factors such as tendon wear, retraction, muscle atrophy, and fatty degeneration. In many cases of chronic massive rotator cuff tears, it can be nearly impossible to bring the torn edges together without putting excessive strain on the repaired tissue, potentially increasing patient susceptibility to mechanical failure. In some cases, the long head of the biceps tendon (LHBT) can be integrated into the cuff repair to not only strengthen the repaired cuff, but also accomplish biceps tenodesis simultaneously. Various LHBT augmentation techniques have been reported. For instance, bridging the LHBT between the tendon and bone can transform an incomplete repair into a complete one and serve as a partial interposition [1]. Similarly, bridging LHBT between the tendons, which replaces the anterior and posterior gap, can facilitate a partial repair [2]. In this study, we introduce a sandwich augmentation technique that incorporates the LHBT into a single-row rotator cuff repair. This approach aims to enhance the thickness of the fully interposed cuff margin to provide better support for the repair.
The Institutional Review Board of Soonchunhyang University Hospital, Cheonan, Republic of Korea, approved this study (No. 2023-10-020).
TECHNIQUE
Arthroscopic procedures were performed with the patient in the lateral decubitus position under general anesthesia, supplemented with a brachial plexus block, if appropriate. Traction of the arm was facilitated using an arm holder, with the shoulder positioned at approximately 30˚ of forward flexion and neutral rotation, which were adjustable throughout the procedure. Standard posterior and anterior portals were used for visualization of the glenohumeral joint and procedures within it. The LHBT was evaluated for any pathology, such as partial tear, subluxation, or dislocation, and debridement was performed. Following the intra-articular procedures, the arthroscope was moved to the subacromial space for further examination. An anterolateral working portal was used for the procedures in this space. After debridement and acromioplasty, the retracted anterolateral portion of the supraspinatus was identified (Fig. 1A), and the LHBT was exposed. Adhesiolysis and mobilization of the torn rotator cuff tendon were performed, followed by footprint preparation of the supraspinatus. To secure the LHBT, tenodesis was performed using a suture anchor within the groove (Fig. 1B). For manipulation and traction, a No. 2 Ethibond stay suture was placed on the proximal end of the LHBT (Fig. 1C), which was then tenotomized at its proximal origin using a radiofrequency device (Fig. 1D). By scratching the synovial surface of the LHBT, we aimed to create an environment conducive to tendon healing after repair. Suture anchors prethreaded with polyethylene sutures were inserted (Fig. 1E). Each strand first passed through the LHBT (Fig. 1F) and then through the rotator cuff margin using a suture passer (Fig. 1G). Each strand passed through the LHBT and rotator cuff simultaneously, and a knot was tied (Fig. 1H). Finally, the LHBT and rotator cuff tissues were attached together to the greater tuberosity, effectively sandwiching them in the rotator cuff footprint (Fig. 1I).
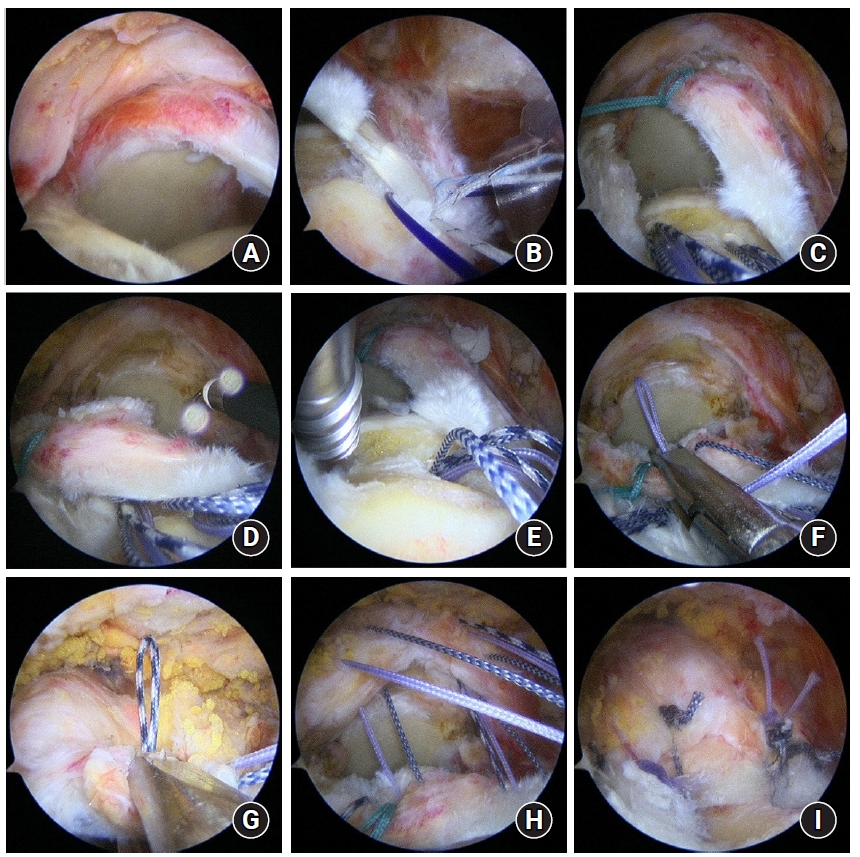
Procedures of arthroscopic rotator cuff “sandwich augmentation” with long head of the biceps tendon (LHBT). (A) The retracted anterolateral portion of the supraspinatus was found. (B) To secure the LHBT, tenodesis was performed using a suture anchor within the groove. (C) For manipulation and traction, a stay suture was placed on the proximal end of the LHBT. (D) LHBT was then tenotomized at its proximal origin using a radiofrequency device. (E) Suture anchors pre-threaded with polyethylene sutures were inserted. (F) Each strand first passing through the LHBT using a suture passer. (G) Each strand then passed through the rotator cuff margin using a suture passer. (H) Each strand passed through the LHBT and rotator cuff simultaneously, and then knot tying was performed. (I) The LHBT and rotator cuff tissues were attached together to the greater tuberosity, effectively sandwiching them in the rotator cuff footprint.
DISCUSSION
The principal finding of this study is that the use of the tenotomized LHBT in the arthroscopic augmentation technique effectively improved structural healing by enhancing the thickness of the cuff margin.
For large or massive rotator cuff tears, the treatment options include either arthroscopic debridement, partial repair, medialization, tuberoplasty, superior capsular reconstruction, or grafting [1,3]. In some instances, tendon transfer or total shoulder arthroplasty, which includes a reverse prosthesis, may be used [4,5]. If the rotator cuff tissue is atrophic and the tendon stump can only be reduced under high tension, techniques such as margin convergence for partial closure, biceps tendoplasty, or local tendon transfer can be utilized [6]. Some surgeons recommend LHBT augmentation when repairing chronic retracted rotator cuffs, because it reduces the likelihood of structural failure and offers enhanced collagen support [1,7].
Cho et al. [1] have published a study on an LHBT augmentation technique similar to ours. The first difference is that biceps tenodesis was not performed in their study. In contrast, our technique initially performs tenodesis within the bicipital groove following a biceps tenotomy. Without initial tenodesis, managing the tension and length adjustment of the augmented LHBT could become challenging. To address this, we first performed tenodesis within the bicipital groove. This makes it easier to adjust the position of the LHBT using a stay suture, thereby eliminating the tension of the tendon caused by muscle contracture in the subsequent procedure. This tension-free state is beneficial for manipulating or moving the tendon during surgery. It also allows accurate targeting of the thread position through the LHBT and the repaired cuff tendon. Furthermore, blocking the variable tension of the augmented LHBT during the rehabilitation period can be advantageous for tissue healing, as it eliminates micromotion on the contact surface of the repaired tendon. During augmentation without tenodesis, the tendon direction should be suddenly angled at the orifice of the groove. This could potentially cause further damage such as a partial tear or complete rupture due to future impingement and could also become a long-lasting source of pain. We believe that tenodesis could prevent this situation. The second difference is that Cho et al.'s technique [1] involves a horizontal arrangement of cuff-LHBT-bone using the Banana suture Lasso. Our technique, on the other hand, involves a vertical arrangement of cuff-LHBT-bone. The strands of the suture anchor are passed from bottom to top through the lateral portal, first through the LHBT and then through the cuff tendon. This allows the cuff’s inferior surface and LHBT’s superior surface to be directly sandwiched. We aim to increase the thickness of the cuff margin to ensure its future strength not to extend cuff length. This technique is particularly useful in patients whose cuff could contact the bare bone but have poor cuff margin quality. It is especially beneficial when there is a high likelihood of future re-tear with the cuff due to poor tissue quality.
Moreover, while Neviaser [8] created a free graft by sectioning the LHBT in the intra-articular portion through an open technique, our technique only directly fixes the proximal portion of the LHBT, preserving its blood supply. This does not disrupt the blood flow to the augmented LHBT, potentially enhancing the healing of the contact surface between the cuff and bone.
Through this method, several advantages can be obtained. First, the tension of the repaired cuff can be reduced due to the thickness of the incorporated biceps. Second, by increasing the thickness of the tendon margin attached to the footprint, the subacromial space can be secured. This minimizes superior migration of the head and prevents cuff damage from mechanical stimulation caused by impingement.
The primary limitation of this technique is the learning curve associated with the procedure, as well as the additional time required to secure the second point of fixation. Furthermore, this procedure is not performed in cases where a massive tear is irreparable.
Using this sandwich augmentation biceps-incorporating rotator cuff repair technique, we achieved positive clinical outcomes and moderate anatomical results. This technique also helped prevent superior migration of the humeral head in cases of large or massive rotator cuff tears. Further research and collection of more case studies are needed to evaluate the long-term effectiveness of this procedure.
Notes
Author contributions
Conceptualization: JBK. Data curation: SJY. Formal analysis: YCC. Funding acquisition: WJK. Investigation: WJK. Methodology: SJY. Project administration: YCC. Resources: JBK. Software: WJK. Supervision: JBK. Validation: JBK. Writing–original draft: SJY. Writing–review & editing: WJK. Visualization: SJY.
Conflict of interest
None.
Funding
The authors would like to thank the Soonchunhyang University Research Fund for support.
Data availability
Contact the corresponding author for data availability.
Acknowledgements
None.