Significant radiologic factors related to clinical outcomes after arthroscopic rotator cuff retear repair
Article information

Abstract
Background
Healing of the tendon itself is not always related to successful clinical outcomes after rotator cuff repair. It was hypothesized that certain radiologic factors affecting clinical outcomes could exist in case of the retear after arthroscopic rotator cuff repair (ARCR) and the radiologic factors could help predict clinical process. The purpose of this study was to identify the radiologic factors associated with clinical outcomes of the retear after ARCR.
Methods
Between January 2012 and December 2019, among patients with sufficient footprint coverage for ARCR, 96 patients with Sugaya classification 4 or higher retear on follow-up magnetic resonance imaging were included. The association between clinical outcomes such as American Shoulder and Elbow Surgeons (ASES) score, Constant score and range of motion and radiologic variables such as initial tear dimension, retear dimension, variance of tear dimension, critical shoulder angle, acromial index, and acromiohumeral distance was analyzed.
Results
Preoperatively, the ASES and Constant scores were 59.81±17.02 and 64.30±15.27, respectively. And at the last follow-up, they improved to 81.56±16.29 and 78.62±14.16, respectively (p<0.01 and p<0.01). In multiple linear regression analysis, the variance of the mediolateral dimension of tear had statistically significant association with the ASES and Constant scores (p<0.01 and p=0.01).
Conclusions
In patients with the retear after ARCR, the variance in the mediolateral dimension of tear had significantly negative association with the clinical outcomes. This could be considered to be reference as relative criteria and needed more sample and mechanical study.
INTRODUCTION
Arthroscopic rotator cuff repair is widely performed, and many studies have reported good clinical results after this procedure [1,2]. However, the rate of retear ranges from 11% to 57% [3-5]. Even though the need for revision surgery due to failure of healing of the rotator cuff has been reported [6,7], healing of the tendon alone is not always related to a successful clinical outcome [5,8]. However, there have been reports of pain relief and return of function even when the healing of the tendons is lacking without revision surgery [1,9,10]. Therefore, understanding the clinical outcomes in patients with rotator cuff retears to identify associated factors is important. The rate and causes of good and poor clinical outcomes after rotator cuff retears are not well established.
Based on the hypothesis that specific radiologic variables could affect clinical outcomes after rotator cuff repairs, we tested and analyzed these radiologic factors for associations with rotator cuff retear clinical outcomes. The radiologic variables tested included initial tear dimension [11,12], critical shoulder angle (CSA) [13], acromiohumeral distance [13] and acromial index (AI) [14]. These were reported as predisposing factors for rotator cuff retear in a previous study and included retear dimension and variance of initial tear and retear dimension. The purpose of this retrospective study was to identify whether the radiologic factors tested are associated with clinical outcomes. The statistically significant radiologic factors could provide a treatment option reference for the patients experiencing retear after arthroscopic rotator cuff repair.
METHODS
This retrospective study was approved by the Institutional Review Board of Wonkwang University Hospital (IRB No. WKUHIRB-2021-04-007). Informed consent was confirmed by the IRB as unnecessary papers.
Study Sample
Between January 2012 and December 2019, a total of 1,171 arthroscopic rotator cuff repairs were performed by a single surgeon. Patient records were reviewed to obtain demographic data, pre- and postoperative clinical scores, range of motion (ROM) values, and radiographic and operative data from the blinded orthopedic surgeon (MSJ). Clinical scores, ROM values, and radiographic data were routinely obtained at the 3-, 6-, 12-, and 24-month follow-up after surgery. When a decision that revision surgery was necessary due to retear of the rotator cuff was made, the data immediately prior to the revision was used as last follow-up data.
The inclusion criteria for this study were (1) patients who underwent arthroscopic repair of rotator cuff tears with sufficient footprint coverage to reduce bias related to the influence of footprint coverage, (2) patients for whom pre- and operative magnetic resonance imaging (MRI) evaluation was possible and consented to, (3) patients with a tear ≥Sugaya classification 4 as observed on postoperative MRI, (4) patients for whom the double-row transosseous equivalent surgical technique (modified suture bridge technique) was used.
Patients in whom footprint coverage could not be achieved due to massive tears, had arthritic changes (glenohumeral osteoarthritis and rotator cuff arthropathy), or had partial thickness tears <Sugaya classification 4 as observed on follow-up MRI were excluded. Those who underwent concomitant subscapularis repair were also excluded. This study included 96 patients who met the inclusion criteria, and the detailed process for patient enrollment is summarized (Fig. 1). The necessity of revision surgery was determined by considering demands and activity level among the patients with poor clinical scores (American Shoulder and Elbow Surgeons [ASES] <70 or Constant score <60) [15,16] for more than 6 months after surgery. In these revision cases, the data before revision surgery were applied. There were no cases of revision due to stiffness and other causes such as infection.
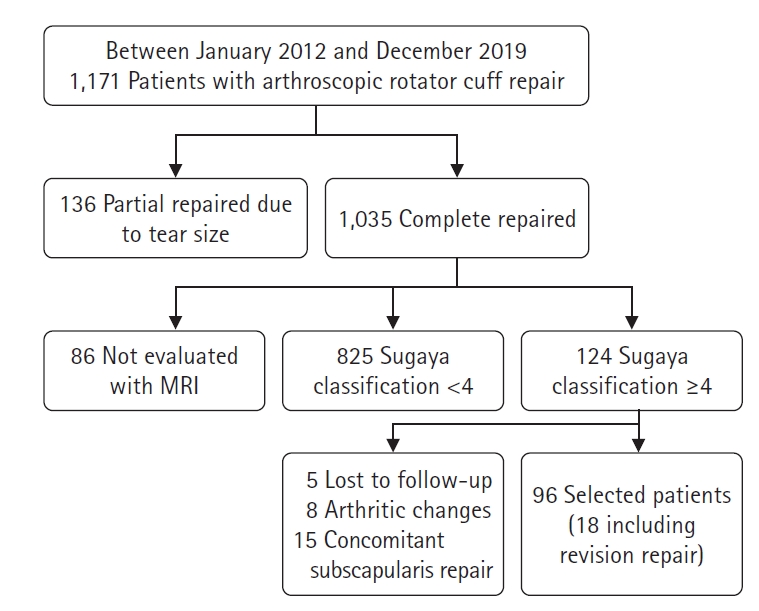
Study flowchart. MRI: magnetic resonance imaging.
Demographics
Demographic variables included sex, age, dominant arm involvement, history of ipsilateral shoulder trauma, presence of inflammatory arthritis (rheumatic arthritis, systemic lupus erythematosus, or ankylosing spondylitis), concurrent diabetes mellitus diagnosis, and positive smoking status. This information is routinely documented at the time of hospitalization.
Clinical Evaluation
Pre- and postoperative ASES scores and Constant scores with an examination of the active ROM, including forward elevation, abduction, external rotation and internal rotation behind the back, were evaluated by the outpatient physiotherapist specializing in orthopedics. For internal rotation, the most proximal point at which the tip of the thumb touched the spinous process was scored based on contiguously numbered groups: T1–12, 1–12; L1–5, 13–17; buttock 18; and greater tubercle of the proximal femur 19 [17].
Radiologic Evaluation
Pre- and postoperative standard radiographs of the shoulder (anteroposterior [AP], true AP, scapular Y, and axillary views) were evaluated. Two orthopedic physicians (MSJ and KLK) independently reviewed the preoperative radiographs to assess the CSA, AI, and acromiohumeral interval (Fig. 2). The CSA was measured as defined by Moor et al. [18], using a line connecting the superior and inferior bone margins of the glenoid and an intersecting line drawn from the inferior bone margin of the glenoid to the most lateral border of the acromion. The AI was measured as the value obtained by dividing the distance from the glenoid plane to the lateral border of the acromion by the distance from the glenoid plane to the lateral aspect of the humeral head. The acromiohumeral interval was measured as the shortest distance from the inferior surface of the acromion to the superior aspect of the humerus in the true AP view [19]. When a subacromial spur was present, the shortest distance between the spur and humeral head was measured.

Measurement of critical shoulder angle (CSA), acromial index (AI), and acromiohumeral interval (AHI) on anteroposterior shoulder radiographs. (A) CSA is formed by a line connecting the inferior with the superior border of the glenoid fossa and another line connecting the inferior border of the glenoid with the most inferolateral point of the acromion. AI is the distance from the glenoid plane to the lateral border of the acromion (GA) divided by the distance from the glenoid plane to the most lateral aspect of the humeral head (GH). (B) AHI is measured as the shortest distance from the inferior surface of the acromion to the superior aspect of the humerus.
Pre- and postoperative MRIs were performed. Khazzam et al. [20] reported that intact repaired rotator cuffs or full-thickness retears can be identified with moderate reliability using MRI after rotator cuff repair, and Iannotti et al. [21] reported that retears primarily occurred between 6 and 26 weeks after arthroscopic rotator cuff repair. Accordingly, postoperative MRI was routinely evaluated with the consent of the patient to identify the condition of the repaired cuff independently of clinical symptoms. MRI was performed at least 6 months (mean, 8.64±2.72 months) postoperatively.
A 3-T imaging unit (Achieva; Philips Healthcare, Best, the Netherlands) equipped with a dedicated shoulder coil (4-channel SENSE shoulder coil, Philips Healthcare) was used to obtain the MR images. The sequences and parameters of the MRI were: axial turbo spin-echo T2-weighted (field of view [FOV], 140×140 mm; repetition time/echo time [TR/TE], 3,800/80; matrix, 256×255; section thickness, 2.0 mm; and intersection gap, 0.2 mm), oblique coronal turbo spin-echo T2-weighted (FOV, 140×140 mm; TR/TE, 3,500–4,000/80; matrix, 350×248; section thickness, 2.0 mm; and intersection gap, 0.5 mm), oblique coronal fat-saturated T2-weighted (FOV, 140×140 mm; TR/TE, 3,500–4,000/80; flip angle, 90°; matrix, 256×255; section thickness, 2.0 mm; and intersection gap, 0.5 mm), and oblique sagittal turbo spin-echo T2-weighted (FOV, 140×140 mm; TR/TE, 5,400–6,000/80; matrix, 232×230; section thickness, 2.0 mm; and intersection gap, 0.5 mm).
Tendon integrity was classified based on postoperative MRI findings proposed by Sugaya et al. [22]: type I, a repaired rotator cuff with sufficient thickness and homogeneous low intensity on each image; type II, sufficient thickness associated with a partial high-intensity area; type III, insufficient thickness without discontinuity; type IV, presence of a minor discontinuity in more than one image, suggesting a small tear; and type V, presence of a major discontinuity on each image, suggesting a medium or large tear. Thus, types I, II, and III represent healing of rotator cuffs, while types IV and V represent retears.
The maximum mediolateral lengths and AP widths of pre- and postoperative tears were measured using the protocol of Davidson et al. (Fig. 3) [23], and variance of tear dimension was calculated by subtracting the preoperative dimension from the postoperative dimension for mediolateral lengths and AP widths, respectively. Two orthopedic physicians (MSJ and KLK) independently reviewed the radiographs and magnetic resonance images to assess the measurement variables. The intraclass correlation coefficient was used to assess interobserver reliabilities for agreement regarding measured values. Correlation was determined to be poor if the coefficient was <0.4, marginal if ≥0.4 and ≤0.75, and good if >0.75 [24].

Measuring pre- and postoperative tears using the magnetic resonance imaging (MRI) protocol of Davidson et al. [23]. (A) Preoperative maximal mediolateral length on T2-weighted coronal oblique MRI view. (B) Preoperative anterior to posterior widths on T2-weighted sagittal oblique MRI view. (C) Postoperative maximal mediolateral length on T2-weighted coronal oblique MRI view. (D) Postoperative anterior to posterior widths on T2-weighted sagittal oblique MRI view.
Statistical Analysis
All continuous variables were tested for normality using the Kolmogorov-Smirnov test. Measurements were expressed as mean±standard deviation with 95% confidence intervals for continuous variables that complied with normal assumptions. The independent t-test or Mann-Whitney U-test were used for categorical variables such as sex, diagnosis of concurrent diabetes mellitus, positive smoking status, involvement of the dominant arm, and involvement of ipsilateral shoulder trauma to identify correlations with the clinical outcomes (ASES score and Constant score). Pearson correlation analysis was used for age, which is a continuous variable.
In univariate analysis of radiologic results, a simple linear regression analysis was used for continuous variables, and significant variables with p<0.05 in the univariate analysis were included in the multivariate analysis. In the multivariate analysis, multiple linear regression analysis was performed in a stepwise manner using variables that showed statistical significance in the univariate analysis. This allowed for the identification of important factors associated with clinical functional scores. Statistical significance was set at p<0.05. Statistical analysis was performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Demographic Data and Clinical Outcomes
The mean follow-up period was 26.91±8.15 months. As indicated in the flow chart (Fig. 1), five cases were lost to follow-up, eight cases of arthritic changes including rotator cuff arthropathy and 15 cases of concomitant subscapularis repair were excluded among 124 patients diagnosed with rotator cuff retear. Clinical and radiologic data from 18 patients who had revision repair surgery were analyzed before revision surgery. Postoperative MRI was performed at an average of 8.64±2.72 months. At the last follow-up, the ASES and Constant scores were 81.56±16.29 and 78.62±14.16, respectively; the ROM was 152.13°±28.81°, 57.59°±18.83°, and 12.41±5.72 points in forward elevation, external rotation, and internal rotation, respectively. The p-values for preoperative and postoperative statistical significance are indicated in Table 1. There was no significant correlation between the clinical scores (ASES and Constant scores) and demographic variables (Table 2).

Clinical outcomes preoperative and at last follow-up

The association of demographic data with clinical outcomes
Radiologic Results
In the univariable analysis, the ASES at the last follow-up was significantly associated with the CSA, retear length (the mediolateral dimension of the retear), variance in the tear width, and variance in the tear length. The Constant score was significantly correlated with the CSA, variance in the tear width, and variance in the tear length (Table 3). Stepwise multiple linear regression analysis was used to identify variables with significant associations with ASES score and Constant score in univariable analyses. Both ASES and Constant scores were significantly associated with the variance in the tear length (Table 4).
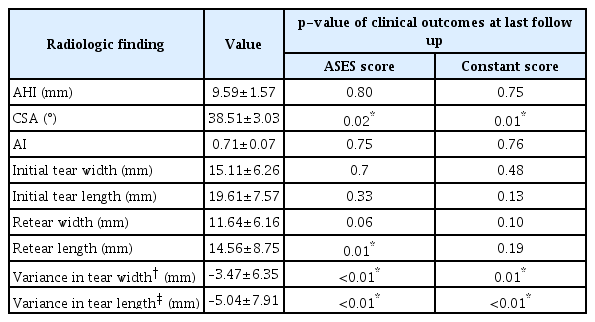
Univariable analysis of radiologic findings associated with clinical outcomes after rotator cuff retear

Multivariable linear regression analysis of radiologic findings associated with clinical outcomes after rotator cuff retear
The multiple regression analysis model for the ASES score was appropriate, F=11.153 (p<0.001) and adjusted R2=0.476, indicating 47.6% explanatory power. The variance in the retear length was B=–0.729 (p=0.002), indicating a 7.29 decrease per 1 mm increase in the tear length variance. Similarly, the multiple regression analysis model for Constant score was appropriate, F=12.685 (p<0.001), and adjusted R2=0.503, indicating 50.3% explanatory power. The variance in the tear length was B=–0.671 (p=0.01), indicating that the Constant score decreased by 6.71 per 1 mm increase in the variance in the tear length (Table 5). The intraclass correlation coefficient indexes of interobserver reliability were 0.91, 0.88 and 0.79 for AHI, CSA and AI, respectively, and were 0.81 and 0.77 for variance in tear width and length.
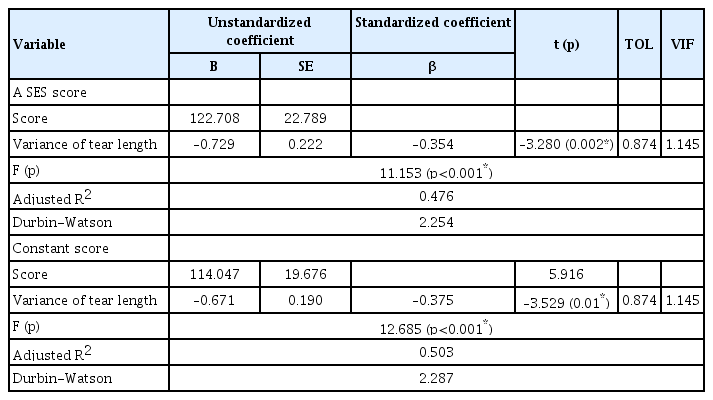
Results of multivariable linear regression analysis (ASES and Constant scores)
DISCUSSION
The results of the present study suggest that the enlarged mediolateral tear size (length) of the rotator cuff have significant negative association with the clinical outcomes of the retear after arthroscopic rotator cuff repair. The explanatory power of the variance of mediolateral tear length associating with ASES and constant score was 47.6% and 50.3%, respectively, which corresponded to a moderate level of more than 40%. Since the explanatory power is not at a high level, these results may be best used as a reference for meeting relative criteria.
As intrinsic anatomical factors, the CSA and AI have been reported to be significant factors in rotator cuff tear. In many studies, larger CSA and AI were reported to be associated with full-thickness tears of the rotator cuff [25]; however, the association with clinical outcomes after surgical rotator cuff repair is not consistent with the general consensus. Kirsch et al. [26] studied the association between the CSA and functional score 24 months after arthroscopic rotator cuff repair and reported that the CSA was not a significant predictor of clinical outcomes. However, Garcia et al. [13] reported that a large CSA was associated with worse postoperative functional outcomes. In addition, Ames et al. [27] reported that a larger AI after rotator cuff repair resulted in a lower satisfaction score, while Lee et al. [28] reported that an increase in the CSA or AI did not negatively affect functional outcomes.
In this study CSA and AI may have been factors affecting retear after rotator cuff repair; however, the analysis revealed no significant associations with clinical outcomes in patients with rotator cuff retear. The high CSA induces overload by increasing the cranially-directed shear force of the supraspinatus, and this mechanical overload of the tendon leads to a degenerative tear in the rotator cuff [29]. We assume that these mechanical effects influenced clinical outcomes; however, more detailed biomechanical study is needed to identify the degree of CSA influence.
Lee et al. [30] reported that the initial size of the rotator cuff tear may be a risk factor for a retear after repair. Gladstone et al. [31] and Wu et al. [32] identified initial tear size as an independent predictor of rotator cuff retear. Especially, in the study by Gladstone et al. [31], the initial tear size was reported to be the only independent predictor of rotator cuff retear in a multivariate analysis. In the present study, the sizes of the initial tear and retear, in both the mediolateral length and AP width, were not significantly associated with the clinical score. However, the variance in the mediolateral length, rather than in the AP width, had significant associations with the ASES and Constant scores.
In a study with a 5-year follow-up after rotator cuff repair, Gulotta et al. [33] found that for every 1 cm increase in initial tear size in the sagittal plane (anterior to posterior) on ultrasonography, the risk of defect increased 1.72 times. However, this group also reported that the risk of defects was not associated with clinical outcomes. These results are consistent with those of the present study. In this study, we evaluated pre- and postoperative magnetic resonance images, which are more precise than ultrasonography, to determine not only the size of the initial tears and retears but also the variance in size of initial tears and retears. Similar to the study mentioned above, the clinical outcome was found to be related more with the variance in the mediolateral length than that in the AP width. Thus, the clinical outcomes after rotator cuff retear may be worse in conditions that aggravate the medial retraction of the defect in the rotator cuff. Based on this, we have extrapolated that the medial and lateral sides must be carefully aligned without excessive tension during the repair of the rotator cuff. Dierckman et al. [34] evaluated the in-vivo tension applied to the rotator cuff tendon positioned at the medial versus lateral footprint during arthroscopic rotator cuff surgery and demonstrated a significant, 5.4-fold increase in tension when the tendon edge was reduced to the lateral as opposed to the medial footprint. Therefore, in cases in which coverage of the lateral footprint is barely possible, a reduction in the medial footprint with an appropriate tension would be better for prevention of medial retraction postoperatively.
Kim et al. [35] measured the dimensions of rotator cuff tears (AP and mediolateral) and the remaining tendinous portion of the rotator cuff in patients with rotator cuff tears and analyzed the relationship between tear dimensions and the remaining tendinous portion of the rotator cuff. These researchers showed that the remaining length of the tendinous portion became shorter as the mediolateral dimension of the rotator cuff tear increased but was not affected by the AP dimension of the tear. In the present study, as the length of the mediolateral tear increased, the remaining tendinous length of the rotator cuff decreased. This may have affected the clinical outcomes; however, these findings should be verified by specific mechanical study and additional studies with larger sample sizes.
There were several limitations to the current study. This study had the inherent weaknesses of a retrospective study. As the influence of concomitant procedures (acromioclavicular joint resection, biceps tenotomy, and biceps tenodesis) were not evaluated, those could have introduced bias. In seven patients with inflammatory arthritis as an underlying disease, there were no direct arthritis findings in the shoulder joint. However, the inflammatory arthritis could affect clinical outcomes indirectly. This study evaluated only patients with rotator cuff repair using the suture bridge technique and had low correlation when other repair techniques were applied. Rehabilitation can also create a bias because the start time of passive and active ROM exercises was personalized according to the degree of patient pain and the condition of the repaired rotator cuff assessed by ultrasound during follow-up. There is a possibility that the result of this study could not be applied universally due to the substantial number of exclusion criteria to reduce bias. Also, since explanatory power of variance in mediolateral tear length associating with ASES and Constant score was only moderate, this result should be used for reference only.
However, despite the retrospective nature of the study, the reduction of bias makes the findings significant. Linear regression analysis was used to reduce selection bias that may occur from dividing groups, and the same variables were demonstrated to have statistically significant results with the two clinical functional scores (ASES and Constant scores). This increased the relevance of the results. In patients with a retear after arthroscopic rotator cuff repair, radiologic evaluation demonstrated that the variance in the mediolateral tear length has significantly negative association with the clinical outcomes. Further prospective and mechanical studies are necessary to identify more specific factors that correlate with clinical outcomes after rotator cuff retear.
Notes
Financial support
None.
Conflict of interest
None.