INTRODUCTION
Calcific tendinitis of the shoulder is a common condition, accounting for 7%–17% of shoulder pain cases [1-3]. It occurs more frequently in women (70% of cases) and among those in their 50s [4]. Calcific tendinitis is a self-limiting condition and can be treated conservatively with rest, physical therapy, oral pain medications like nonsteroidal anti-inflammatory drugs (NSAIDs), calcium deposit needle lavage, steroid injection, and extracorporeal shock wave therapy (ESWT) [5-9]. There is still some controversy about the optimal treatment modality for calcific tendinitis of the shoulder. Ultrasound (US)-guided techniques, such as barbotage and needle decompression for calcific tendinitis, have been reported [5,8,10-12], and most have demonstrated good outcomes. Some studies have reported that the initial size of calcium deposits do not affect the clinical outcomes in patients receiving conservative treatment [13,14]. However, treatment using US-guided barbotage with a needle has not yet been established as a standard technique.
This study analyzed the clinical and radiological outcomes of US-guided barbotage using a spinal needle and subacromial steroid injection for calcific tendinitis of the shoulder. We also investigated the influence of initial calcium deposit size on clinical outcomes. We think in patients with calcific tendinitis of the shoulder, US-guided barbotage using a spinal needle and subacromial steroid injection can yield satisfactory results both clinically and radiologically.
METHODS
The study was approved by the Institutional Review Board/Ethics Committee (IRB No. CR321012), and informed consent was obtained from all participating subjects.
We evaluated 36 patients with calcific tendinitis who were treated with US-guided barbotage and subacromial steroid injection from January 2018 to December 2019. All subjects experienced shoulder pain for more than 3 months, irrespective of initial calcium deposit size. Patients with other shoulder diseases, such as rotator cuff tears (by US), glenohumeral joint arthritis, or infection, and those with a history of US-guided therapy for ipsilateral shoulder (steroid injection, barbotage, needle decompression), ESWT, or surgery were excluded from the study.
Clinical and Radiological Evaluation
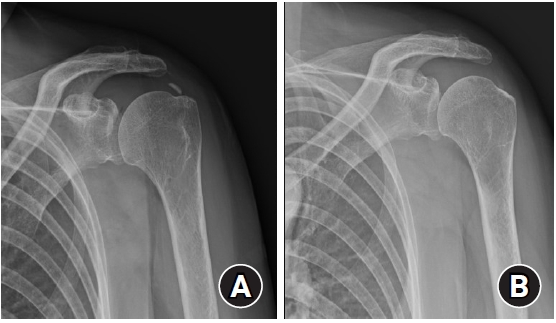
Clinical and radiological evaluations were performed before the procedure and at 6 weeks, 3, 6, and 12 months after the procedure. Routine radiological evaluations were performed using the shoulder anteroposterior view in neutral, axial, and Rockwood view. The Gärtner classification was used to assess calcific deposits the radiographs [15]. The calcific deposit size was determined at each follow-up visit using the longest measurement in any direction.
Clinical evaluations were performed using the American Shoulder and Elbow Surgeons (ASES) scores, Constant scores, and visual analog scale (VAS) for pain scores recorded at each visit. We analyzed the relationship between initial calcific deposit size and each outcome variable (VAS, ASES, and Constant scores) at different time points.
US-Guided Barbotage and Subacromial Steroid Injection
All US-guided barbotage and subacromial steroid injections were performed aseptically by a single orthopedic surgeon. First, a diagnostic US was performed, during which the biceps tendon, rotator cuff, and AC joint were checked for lesions. We also checked the location and characteristics of calcific deposits. The procedure was done in a sitting position. Examination was conducted with the patient's arm in a modified crass position. The skin was cleaned with 10% iodopovidone solution several times, aseptically draped, and treated with lidocaine for local anesthesia. After confirming the position of the calcium deposit, the needle was inserted in the short axis view. The calcific deposit was punctured with an 18-gauge needle. After confirming that the needle tip was located in a calcific deposit, it was aspirated with a 10-mL syringe, and if possible, this was repeated several times. Using a spinal needle, the deposit was punctured multiple times to achieve decompression. The final step was an injection of triamcinolone 40 mg/1 mL, hyaluronidase 0.5 mL, Ropiva 3 mL into the subacromial space under US guidance with an 18-gauge needle. All patients were prescribed 7 days of oral NSAIDs, with no specific activity restrictions.
Statistical Analysis
The categorical data are reported as numbers with percentages for proportions. Continuous data are reported as median (interquartile range), and the Shapiro-Wilk test was used to determine normal distribution. A one-way analysis of variance (ANOVA) with repeated measures and Greenhouse-Geisser correction was used for patient data (with US-guided barbotage and steroid injection for calcific tendinitis of the shoulder), calcium deposit size (mm), VAS, ASES, and Constant scores recorded at different time points (before surgery, 6 weeks, 3, 6, and 12 months after the procedure). Post hoc mean comparisons with the Scheffé least significant difference test in Prism test were performed to identify time points that exhibited significant differences. Spearman's correlation analysis was performed to determine the correlation between the initial calcific deposit size and the clinical outcomes at each time point. A p-value <0.05 was considered statistically significant. R ver. 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria) was used to create a spaghetti plot and mean profile plot. All statistical analyses were conducted using the IBM SPSS 23.0 (IBM Corp, Armonk, NY, USA).
RESULTS
Thirty-six patients were treated with US-guided barbotage and subacromial steroid injection. Of them, 31 were women, and 5 were men. The average age of the subjects was 58 years (range, 53–61 years). While 28 patients received the injection in the dominant arm, 8 received it in the non-dominant arm. In the initial radiological evaluation, based on Gärtner classification, 18 patients had type I, while 13 had type II, and 5 had type III calcifications. The average initial calcific deposit size was 13.5 mm (range, 10.0–20.1 mm), VAS score was 6 points (range, 5.0–9.0 points), ASES score was 56 points (range, 51.5–73.5 points), and Constant score was 63 points (range, 48.0–75.0 points) (Table 1). None of the patients experienced any complications after US-guided barbotage and subacromial steroid injection.
Changes in calcific deposit size and the VAS, ASES, and Constant scores after US-guided barbotage and subacromial steroid injection were significant (Table 2, Fig. 1). Furthermore, all of the above variables showed a statistically significant changes from 6 weeks after procedure (Table 3). Of the 36 patients, one underwent arthroscopic calcification removal 4 months after the initial injection. The calcific deposit size in this patient decreased from 18.08 to 12.84 mm in 6 weeks, and VAS score dropped from 6 to 3 points. However, after 3 months, while the calcific deposit was still the same size, VAS score increased to 6 points. Although conservative treatment was recommended, further conservative treatment was refused; surgical treatment was explained and the patient consented to the procedure. After surgical treatment, pain was reduced and calcium deposits were not observed on postoperative X-ray. We found no significant relationship between initial calcific deposit size and outcome variables (VAS, ASES, and Constant scores) at different time points (Table 4).
DISCUSSION
Confirming our initial hypothesis, the study findings demonstrated reductions in pain and calcium deposit size in patients with calcific tendinitis of the shoulder who were treated with US-guided barbotage and subacromial steroid injection. Moreover, the initial calcific deposit size showed no significant correlation with clinical outcomes at each time point.
Until now, several conservative treatments have been used for patients with calcific tendinitis of the shoulder. ESWT has shown short-term and long-term clinical improvements in 53%–71% and 66%–91% of patients, respectively [15-18]. When introduced, barbotage was carried out under fluoroscopic guidance [19,20]. However, this method had the disadvantage of radiation exposure and difficulty accurately targeting calcium deposits. More recently, barbotage is increasingly being performed under US guidance, with no risk of radiation and more accurate localization of calcium deposits [10,21]. Hence, more US-guided procedures are being performed on patients with calcific tendinitis with good clinical success rates [5,6,11,14,22,23].
In a study of the US-guided needle procedure in a patient with calcific tendinitis of the shoulder, symptoms improved after 3 months, and a significant decrease in deposit size was observed after 6 months [5,23]. However, in our study, statistically significant improvement in symptoms and a decrease in deposit size were observed 6 weeks after the procedure. Unlike other studies that used an 18-gauge needle for multiple puncture decompression, we used an 18-gauge needle for aspiration and then performed multiple puncture decompression using a spinal needle, which can be used to perform decompression at deeper and more difficult angles. On the same day, a decrease in the calcific deposit size was confirmed by US; as deposit size decreased, symptoms improved.
In one study, barbotage was reported to yield better outcomes in cases with ill-defined calcifications (e.g., Gärtner type II or III classification) [11]. In another study, based on the Gärtner classification, shoulders were divided into two groups: (1) type I and (2) type II and III calcifications. The two groups presented no statistically significant differences in Constant and University of California Los Angeles scores [13]. Consistent with the latter study, we found good clinical outcomes in all patients irrespective of their Gärtner classification. Therefore, it appears that the degree of decompression of calcific deposits affects the outcome of the procedure more than patient Gärtner type.
In this study, there was no significant correlation between initial calcific deposit size and clinical outcomes at each time point. These findings were consistent with Cho et al. [13], showing no statistically significant differences in Constant and University of California at Los Angeles (UCLA) scores between calcific tendinitis patients with large- and small-sized initial calcific deposits and who received conservative treatment. Kim et al. [14] reported no significant correlation between initial calcific deposit size and clinical outcomes in calcific tendinitis patients receiving ESWT and US needle compression.
Our study has several limitations. First, there was no control group in this study. Although US-guided needle treatment had sufficiently good outcomes, a comparison with other conservative or surgical treatments would make the findings more robust. Second, as mentioned before, most study subjects were chronic patients since they had already received conservative treatments like oral medication and physical therapy at other hospitals, which had failed. Thus, in a wider population, treatment satisfaction may be increased. Given the subjective nature of the evaluation, clinical outcomes such as the ASES, Constant, and VAS scores may also have been overestimated in these subjects compared to other patients. Lastly, the number of patients in this study was small. A study with a larger sample size is needed to validate our findings. In patients with calcific tendinitis of the shoulder, US-guided barbotage using a spinal needle and subacromial steroid injection can produce clinically and radiologically satisfactory results.