INTRODUCTION
Surgical treatment of a massive rotator cuff tear (RCT) is always a challenge for orthopedic surgeons [1]. Irreparable RCTs are characterized by a lack of mobility, which precludes complete repair of native rotator-cuff tendons on the footprint [2]. Poor tissue quality of a retracted rotator cuff precludes mechanically sufficient repair, and unavoidable tension may predispose the tissue to repair failure [3]. Conventional techniques for soft-tissue release are often insufficient for tension-free repair, and the failure risk may increase if excessive tension is applied during the repair process [4-6]. Several treatment options, such as rotator-cuff augmentation with allografts, biceps rerouting, tendon transfer, and reverse total-shoulder arthroplasty have been proposed to deal with these consequences of an irreparable RCT [2,7-12]. A superior capsular reconstruction technique introduced by Mihata et al. [13] has been widely performed and clinical outcomes have been reported. However, the technique suffers from a long operative duration, donor-site morbidity, and technical difficulties [14]. Biceps rerouting cannot be used in cases of a completely torn long head of the biceps tendon [14]. Another viable option may be a bridge graft that spans the residual stump of the rotator cuff and tuberous bone [11,15-17]. This configuration is typically used to decrease repair tensions for irreparable RCTs [15,16].
Several systematic reviews have reported that the bridging procedure may provide superior tendon healing, although the clinical outcomes of the bridging grafts were not significantly better than those of patch augmentation [15-17]. Another systematic review reported that a bridging graft merely closes a defect with no possibility of restoring the muscle-tendon unit’s length-tension relationships. The graft would serve as a primary load-bearing structure between the rotator cuff and the humerus [16]. Although the biocompatibility of artificial grafts and xenografts that can be used for patch augmentation is spreading with technological advances, these materials run the risk of causing inflammatory reactions and potentially resorbing over time [18]. A modified Mason-Allen stitch can hypothetically fix a long tendon autograft securely to the rotator-cuff tissue, and the other side of the tendon may be robustly anchored to the humeral bone with Bio-Tenodesis screws. Various tendons were considered for the autograft, but plantaris, which can be harvested without changing the lateral position for arthroscopy, is relatively easy to harvest, and is an effective choice for passing the rotator cuff, was judged to be the most suitable. This study reports the clinical and radiological outcomes of patients who underwent bridging grafts with a long tendon graft for an irreparable RCT.
METHODS
This study was approved by the Institutional Review Board of Yeungnam University Hospital (No. YUMC 2019-05-017). The requirement for informed consent was waived because of its retrospective and observational nature. All methods were carried out in accordance with national guidelines and regulations. We performed a retrospective study of a case series of irreparable RCT repairs performed by a single surgeon (SGP) from June 2017 to January 2020 using arthroscopic bridging graft procedures and a postoperative rehabilitation protocol.
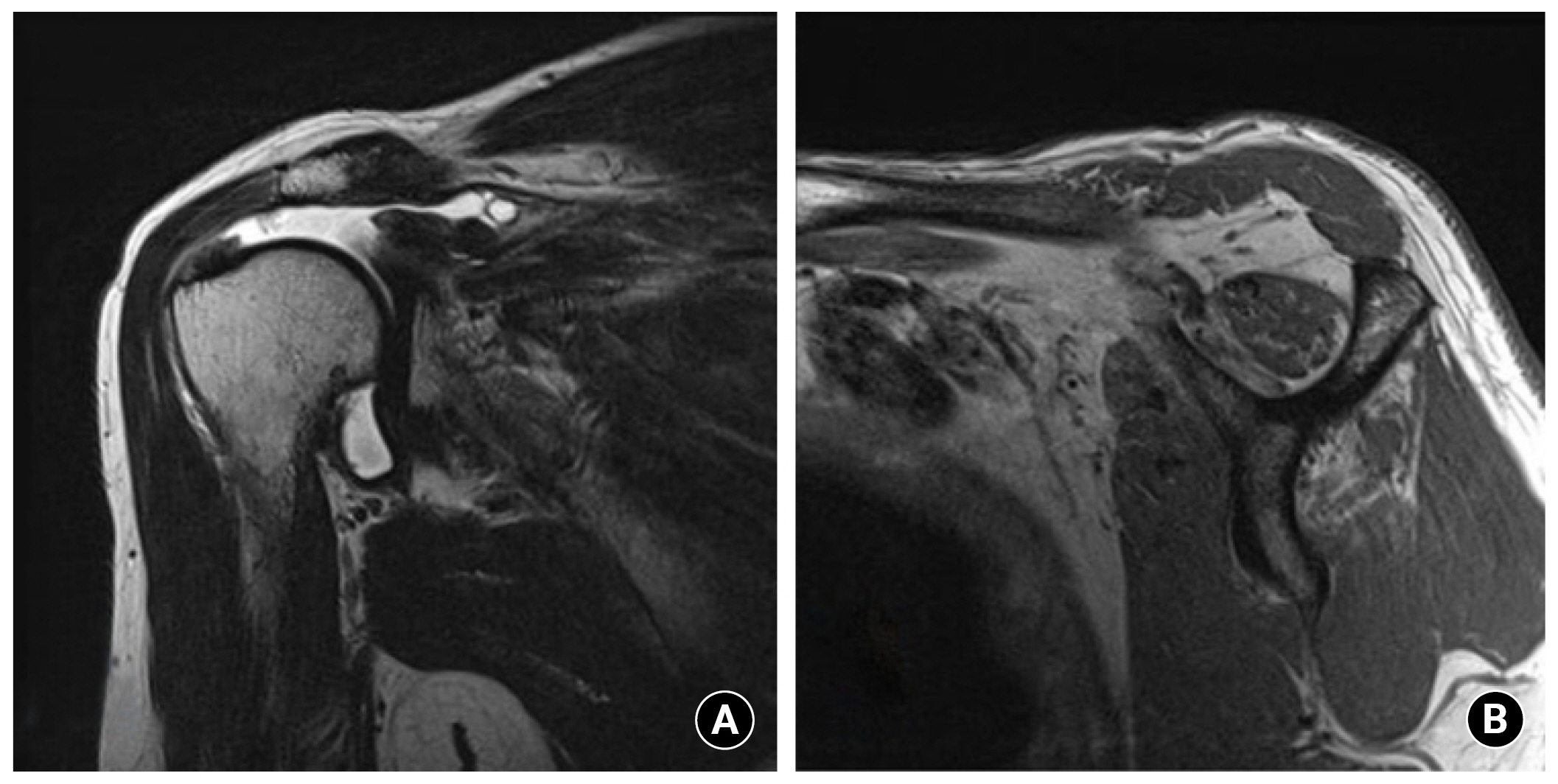
An arthroscopic bridging graft with a modified Mason-Allen stitch using a tendon autograft was indicated for patients diagnosed with an irreparable RCT. The findings of preoperative magnetic resonance imaging (MRI) had to be consistent with an irreparable RCT, with a full-thickness medial retraction greater than 5 cm, grade 3 or greater fatty infiltration of the supraspinatus, and grade 2 or greater change of the infraspinatus on T2-weighted sagittal oblique imaging (Fig. 1) [1]. During diagnostic arthroscopy, the irreparability of the tears was confirmed by the inability of the torn edge of the rotator cuff to attach to the medial margin of the footprint with less than 30 N of tension after maximum mobilization [5]. All surgeries were performed by one surgeon (SGP), who also measured the tension.
Exclusion criteria included glenohumeral arthritis or inflammatory arthropathy based on preoperative radiographs and/or MRI, a rotator cuff that was reducible to the medial footprint under appropriate tension, a RCT with complete subscapularis tendon tear (Lafosse types IV and V) [19], and incomplete follow-up data or MRI evaluation. A total of 13 patients met the study criteria.
Operative Technique
The operative technique described in a technical note previously reported by the authors was used in this study [20]: (1) intra-articular and subacromial debridement, (2) plantaris tendon harvesting and graft preparation, (3) plantaris graft fixation, and (4) final repairable rotator-cuff repair. As detailed explanations with videos and figures describing the technique are provided in the technical note, here we focus on describing the plantaris tendon harvesting and the Mason-Allen suture process [20].
Plantaris tendon harvesting and graft preparation
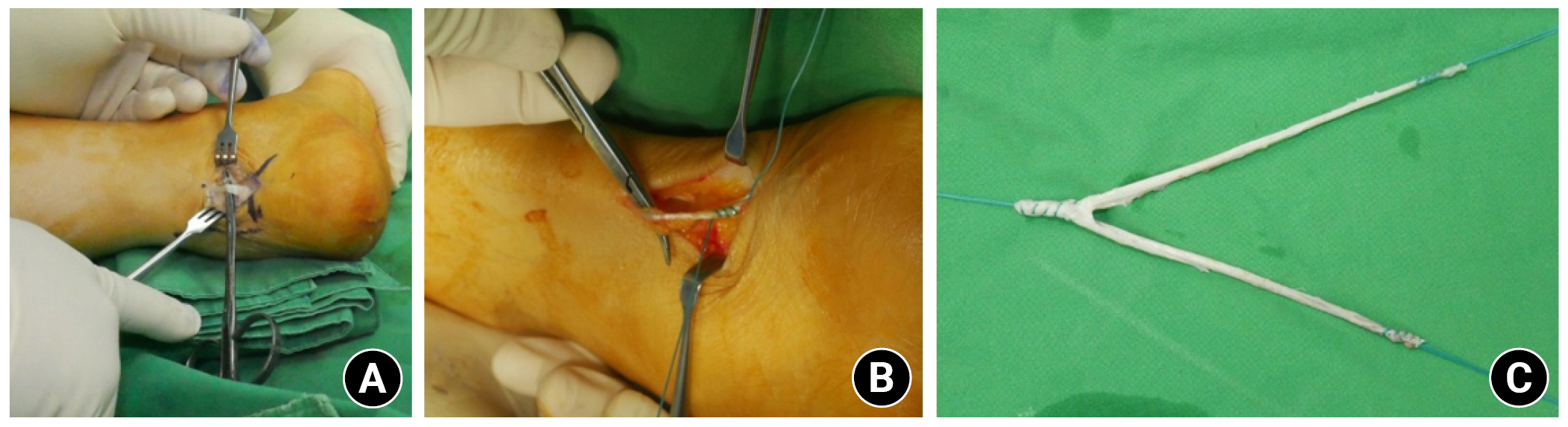
First, the plantaris tendon on the opposite side of the shoulder to be operated on was harvested. After making a 3 cm incision on the skin covering the distal portion of the plantaris tendon, blind subcutaneous dissection was performed until the tendon was reached (Fig. 2A). After the distal insertion of the plantaris tendon was transected, the distal portion of the tendon was prepared for stripping with a No. 2 Ethibond suture (Ethicon) (Fig. 2B). The tendon stripper was advanced slowly and proximally until the muscle-tendon connection was severed and the tendon was retrieved. Approximately 30 cm of the tendon (diameter of approximately 3 mm) was harvested. The tendons were then folded into a Y-shaped graft 15 cm long and the three ends were pre-ligated with Ethibond or FiberWire sutures (Fig. 2C).
Mason-Allen suture using plantaris tendon
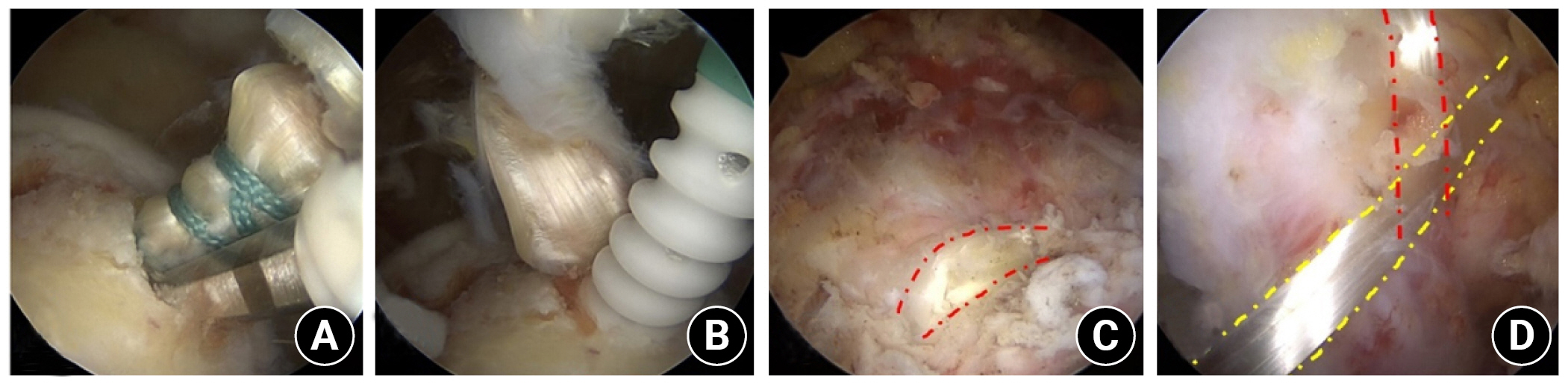
After routine bursectomy and preparation of the footprint of the greater tuberosity, a cannulated reamer 6.5 mm in diameter was passed through the portal to drill a hole for Bio-Tenodesis screw and the folded end of the Y-shaped graft. The folded end of the graft was fixed into the hole with SwiveLock (Arthrex) Tenodesis bicomposite anchors (Fig. 3A and B). A BirdBeak suture passer (Arthrex) was inserted along the posterior edge of the irreversible portion of the tear, 5 to 10 mm more proximal than a conventional suture site. First, one limb of the harvested graft was passed through the cuff in the articular-to-bursal direction. The passed limb of the tendon was retrieved through the posterior portal. For the second passage, the BirdBeak passer was reloaded with thread and passed through the cuff 1 cm anterior to the first passage, and the limb retrieved through the posterior portal was passed in the bursal-to-articular direction by the same method. Next, a transverse loop was made in the bursal side of the cuff (Fig. 3C). For the third passage, the passed graft limb should be situated at the articular side of the cuff. After that, the limb can be passed from the articular-to-bursal direction to form a modified Mason-Allen stitch (Fig. 3D) [9]. A lateral pilot hole was made using a punch at a point where no excessive tension was applied to the rotator cuff. The two FiberWire strands threaded to the first limb of the graft were loaded through the Bio-SwiveLock eyelet. The first limb of the graft was then engaged in the desired position. The procedure was repeated with the other graft limb while moving anteriorly to the anterior edge of the irreparable portion of the cuff tear to be grafted.
Postoperative Rehabilitation
After surgery, the shoulder was immobilized for 6 weeks in a sling with an abduction brace. Only exercises of the elbow, wrist, and hand were allowed for the first 4 weeks. Passive range of motion (ROM) exercises began 4–6 weeks post-surgery, and active training was initiated after 6 weeks. Daily activities, including overhead lifting, were allowed after 12 weeks, with a return to a full range activities after 6 months.
Clinical and Radiographic Evaluations
Clinical results were evaluated before and after surgery using subjective and objective outcome measures at 12 and 24 months, and at the latest follow-up. The mean follow-up duration was 36.2 months (range, 24–53 months), with a minimum of 2 years. Subjective outcome measures included the visual analog scale (VAS), American Shoulder and Elbow Surgeons (ASES), and Disabilities of the Arm, Shoulder, and Hand (DASH). Objective outcome measures included active ROM, including forward flexion, abduction, external rotation at 90° of shoulder abduction, and Constant-Murley scores. For radiographic evaluation, 11 of the 13 patients underwent standardized MRI examinations (MAGNETOM Tim Trio, Siemens). Due to the presence of coronary stents, the other two underwent ultrasonography before surgery and a minimum of 2 years after surgery. Radiologic evaluations were performed approximately 2 years after surgery. Ultrasound imaging was performed and interpreted by a musculoskeletal radiologist with 20 years of experience. The radiological examinations were reviewed using the Picture Archiving and Communications System (Marosis, Infiniti) in a blinded fashion by two independent physicians; one (JKY) was a musculoskeletal radiologist and the other (HGS) was an orthopedic surgeon with 5 years of experience. The physicians identified both the native rotator-cuff tendon and the graft.
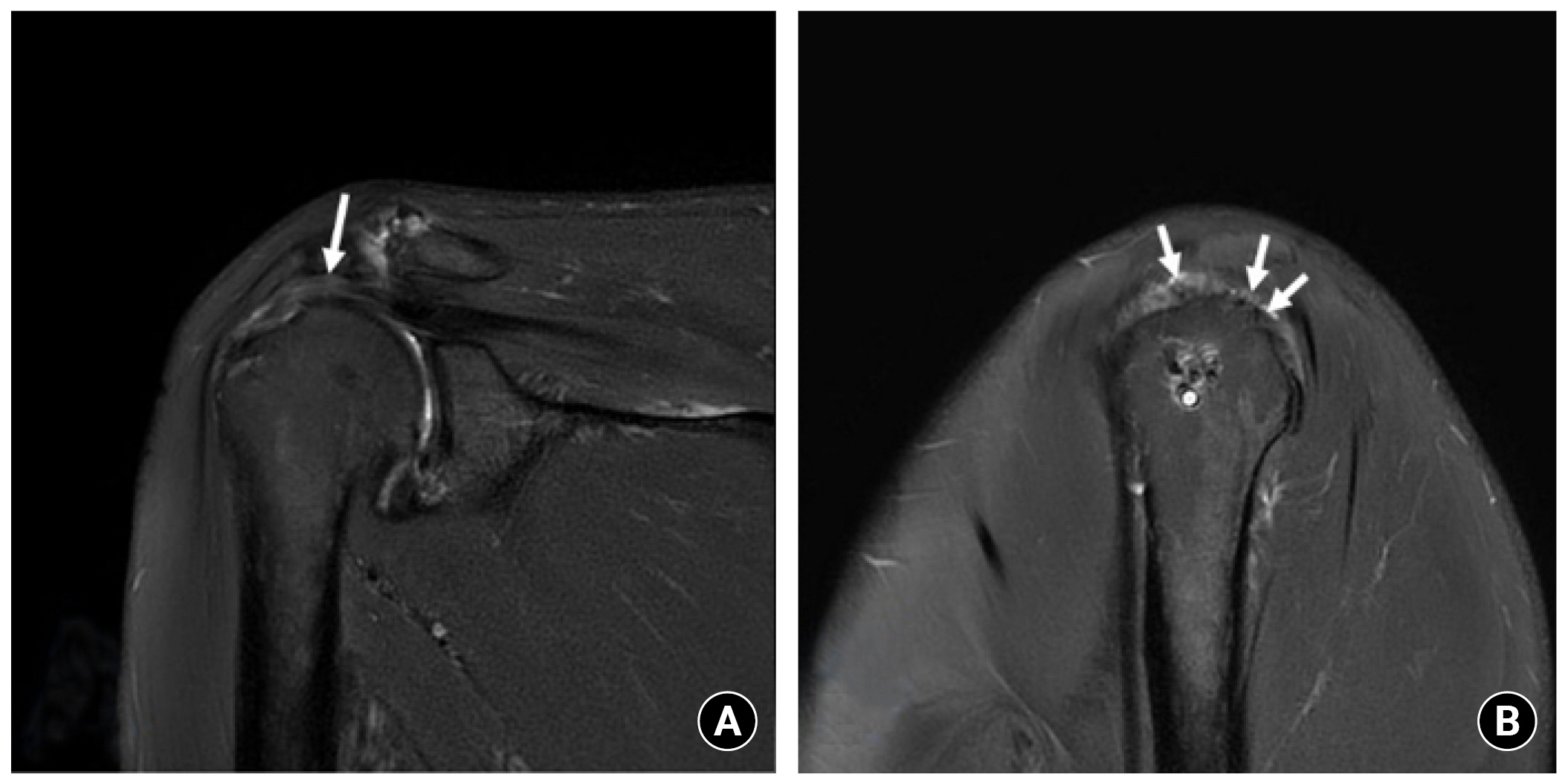
The repairs were classified as “intact,” “partially failed,” or “failed” based on the number of interposed tendons found in the interval between the torn edge of the remnant rotator-cuff tendon medially and the footprint of the rotator cuff laterally. An “intact” construct was indicated by at least 3 of the 4 interposed tendons remaining in tension in the interval or by tendons that were transformed into the membranous patch with no visible defects at the tendon-graft and graft-bone interfaces (Fig. 4). “Partially failed” was indicated by one or two intact tendons in the interval. “Failed” meant a full-thickness defect with no working interposed tendons attached to the native tendon and humeral footprint. Supraspinatus muscle atrophy and the degree of fatty infiltration in the supraspinatus and infraspinatus muscles were measured in most lateral T2-weighted oblique sagittal images, where the scapular spine was in contact with the scapular body (the “Y-view”). Supraspinatus atrophy was divided into three grades based on MRI quantitative evaluation of the occupation ratio (R) described by Rulewicz et al. [21] (grade I, 1>R≥0.6; grade II, 0.6>R≥0.4; and grade III, R<0.4). The degree of fatty infiltration was categorized as a Goutallier index modified to use MRI by Lippe et al. [22].
RESULTS
The mean age of the patients was 68.5 years (range, 58–79 years). The mean tear size was 44.1 mm×44.5 mm (i.e., the medial-to-lateral defect times the anterior to posterior distance described by Davidson et al. [23]. In 12 of the 13 patients, the biceps tendons were ruptured and difficult to find. A tenotomy was performed in one patient with an intact tendon of the biceps brachii. A summary of the demographic characteristics and preoperative evaluations is provided in Table 1.
Statistically significant improvements were seen in all measured functional scores at the final follow-up: VAS (4.9±1.8 to 1.9±1.7, P=0.003), Constant-Murley score (60.2±19.0 to 74.5±9.1, P=0.01), ASES (57.8±17.1 to 82.7±11.5, P=0.002), and DASH scores (32.9±15.6 to 12.3±7.4, P=0.001). Forward flexion (132.3°±44.2° to 149.6°±30.7°, P=0.003), abduction (121.5°±45.4° to 145.8°±25.2°, P=0.009), internal rotation (68.5°± 20.8° to 75°± 12.2°, P=0.325), and external rotation (50.4°±17.5° to 78.1°±17.5°, P<0.001) were also improved post-surgery compared with the preoperative range. However, there was a statistically significant difference only in the forward flexion and external rotation measurements. Table 2 lists the improvement in clinical outcomes at final follow-up.
MRI or ultrasonography was performed 2 years after surgery to verify the integrity of each graft; the interposed tendons were intact in 12 of the 13 patients. Only one patient had a partial failure of the interposed tendons. The patient with a partial failure was satisfied at their last clinical follow-up because their motion limitation and pain were significantly relieved. No harvest-site morbidity was reported in any patients. Table 3 lists the radiological and clinical outcomes at the final follow-up.
DISCUSSION
This case series of 13 consecutive patients who underwent arthroscopic bridging graft for irreparable RCT with a modified Mason-Allen stitch and a tendon autograft showed positive clinical and radiological outcomes. Of the 13 patients, only one (7.7%) experienced failure, in a case that was evaluated as “partially failed.” On follow-up MRI of the patient with partial failure, one of four strands of imposed tendon rupture was confirmed, but the clinical outcome was relatively positive. For this patient, ultrasonography was used to monitor the progression of the partial rupture at every outpatient follow-up visit, but the rupture did not progress, and the patient was satisfied with the clinical outcome.
Successful surgical remedies for a massive irreparable RCT continue to present significant clinical challenges. Primary repair of a massive RCT is likely under at least some degree of tension despite releases, and unavoidable tension on the construct may predispose the patient to pain and repair failure [4-6,24]. For a massive RCT in which primary repair is impossible, various procedures such as muscle transfer and superior capsular reconstruction have been devised, but each has its limitations.
Latissimus dorsi muscle transfer in some young patients may improve external rotation. In patients who underwent a latissimus dorsi transfer procedure, functional scores and ROM improved at both the short-term and long-term follow-ups of >9 years on average [25,26]. This finding is similar to the results of our study using a bridging graft. However, latissimus dorsi transfers in patients with a ruptured subscapularis resulted in poor clinical outcomes and a high complication rate [25].
A superior capsular reconstruction technique has been widely reported, but long-term results are not available; issues regarding failure, graft elongation, persistent superior migration of humeral head, and suture anchor loosening are under debate [27-29]. Denard et al. [29], who used superior capsule reconstruction for irreparable RCTs, reported that ASES scores improved from 43.6 to 77.5 and pain decreased from 5.8 to 1.7. They also reported a 6.8% complication rate. ASES scores improved from 56.9 to 82.7, pain decreased from 4.9 to 1.9, and the complication rate was 14.2%.
The biodegradable subacromial balloon is a relatively new option, but long-term follow-up data are lacking [30]. Senekovic et al. [31] reported on 24 patients who had received a subacromial balloon for an irreparable RCT. At 60 months postoperation, 84.62% of the patients showed a clinically significant improvement, and improvement in ROM was noted in 75% of the subjects. A systematic review [30] described subacromial balloon spacer placement as a minimally invasive and a technically simple procedure with low rates of perioperative complications and favorable outcomes at a limited short-term follow-up.
According to available systematic reviews on patch augmentation and bridging grafts for massive RCTs, despite the tendency to create a more severe tear, bridging grafts exhibit a high healing rate due to the low tension of the repair construct. However, the clinical outcomes were not significantly superior to those for patch augmentation, suggesting that a bridging procedure may provide superior tendon healing but may not necessarily improve function [15-17]. Ono et al. [16] suggested that this may be caused by the fact that a bridging graft merely “closes a hole” without attempting to restore the length-tension relation of the functional, contractile, musculotendinous unit, which may provide a more favorable biomechanical vector for the deltoid muscle.
We hypothesized that an arthroscopic bridging graft for an irreparable RCT with a modified Mason-Allen stitch using a tendon autograft could be used to decrease the tension on the repair of an irreparable RCT and restore the length-tension relationship of the musculotendinous unit. Modified Mason-Allen stitches, with the use of the plantaris tendon securely anchored to the relatively healthy proximal portion of the remaining rotator cuff—and the other side of the graft—could be robustly fixed to the humeral bone with bioabsorbable interference screws. Consequently, the grafts were designed to withstand the rotation and tension stresses of the rotator cuff and may transport force couples from the rotator cuff to the humeral head in a manner similar to that of healthy rotator-cuff tendons. The bridging graft technique produced similar clinical outcomes while providing superior biomechanical advantages that other procedures, such as latissimus dorsi and superior capsule reconstruction, could not provide.
Mori et al. [32] compared a fascia lata autograft group and a partial repair group. The study reported that the fascia lata autograft group had significantly superior clinical outcomes and a lower re-tear rate. The use of a GraftJacket Max graft on 16 patients, evaluated by Bond et al. [33], showed significant postoperative improvement in University of California, Los Angles scores. The outcomes in our study were similar. Awad et al. [34], who used an acellular dermal matrix in 49 patients, reported significant improvements in both Western Ontario Rotator Cuff and Disabilities of the Arm, Shoulder and Hand scores at a mean follow-up of 5.3 years. Comparing the results of this case series with that of previous studies, arthroscopic bridging graft for irreparable RCT with a modified Mason–Allen stitch produced outcomes comparable to those of other techniques.
Advantages and Disadvantages of Plantaris Tendon
The nature of materials that would be appropriate for this procedure is an important element of this study. An ideal graft must be securely anchored to the remaining rotator-cuff tissue as it must develop a robust bony attachment at the footprint to withstand rotation and tension stresses. In addition, it should promote cell recruitment and adherence, facilitating tendon regrowth. To satisfy these conditions, we proposed an autograft of the plantaris tendon that can provide sufficient length and tension and can readily engraft [35]. Plantaris autografts have several potential advantages: the tendon is easy to harvest and has a strong potential for biological superiority compared with allograft materials that may enhance healing with no inflammatory reactions. The width of the tendon (approximately 3 mm) makes it easy to pass through the rotator cuff, and its length (approximately 30 cm) allows for complex stitches such as modified Mason-Allen sutures [36]. It also costs less than allografts. The disadvantages of this techniques include tedious graft preparation, longer operating time, the absence of the plantaris tendons, and possible donor-site morbidities. Because harvesting and tendon preparation are necessary, the operating time inevitably increases by approximately 30 minutes. Although excluded from this study, failure in a patient who underwent a bridging graft using the semitendinosus tendon due to lack of plantaris was confirmed by MRI at 2 years. No further surgery was performed because the patient refused. No morbidity at the harvest site was reported in any case.
Limitations
Our study had some limitations. First, the retrospective design of this study could introduce selection bias and potential confounding variables. Second, this study had a relatively low statistical power due to the short-term follow-up and small sample size. Additional follow-up observations are needed to determine if this method does not completely cover rotator-cuff defects. However, the short-term clinical outcomes at our institution have shown promising results. Larger studies with long-term follow-ups are required to further evaluate the efficacy of this technique.
CONCLUSIONS
This case series shows that an arthroscopic bridging graft for irreparable RCTs using a modified Mason-Allen stitch and a plantaris tendon autograft resulted in improved short-term radiological and clinical outcomes. Graft integrity in most patients was maintained for up to 2 years after surgery. The technique can be considered for the treatment of a massive RCT. Further studies and follow-ups are required to determine the success of this technique.