INTRODUCTION
The acromioclavicular (AC) joint is a diarthrodial joint in the shoulder between the distal clavicle and the acromion. The AC joint is stabilized by muscular and ligamentous structures including the deltoid and trapezoid muscles and the capsular, AC, and coracoclavicular ligaments [1]. AC joint separation is common among athletes and occurs following a traumatic injury to the shoulder [2]. This injury is roughly 10 times more frequent in men than in women [3]. AC joint separation accounts for 9% of all shoulder injuries but 40% of all sports-related injuries [4,5]. The mechanism of injury is typically a fall or a direct blow to the shoulder with the arm adducted [6]. Many classifications have been proposed to describe AC joint dislocations. The Cadenat classification was published in 1917, followed by the Tossy classification in 1963 and the Rockwood classification in 1984 [7,8]. The Rockwood classification uses plain radiographs to categorize AC joint dislocations into six grades of severity and nature of ligament injuries and joint dislocation. The grades range from mild sprain in grade I to complex ligament rupture and dislocation in grades IV to VI [3]. The higher is the classification of the injury, the worse is the prognosis.
Recent reports show that intra-articular glenohumeral pathologies (IAPs) often accompany low-grade AC joint dislocations, which challenges the notion that they are only seen in high-grade injuries [6]. Despite this, there is a lack of comprehensive studies on the occurrence of labral tears alongside AC joint dislocations. To fill this gap, our systematic review sought to accomplish two main objectives. First, we evaluated the prevalence of labral tears in AC joint dislocations. Second, we attempted to identify risk factors that may contribute to this association, such as age and grade of AC joint dislocation. We hypothesize that labral tears are a commonly overlooked pathology that may frequently co-occur in both low- and high-grade AC joint dislocations. We also suspect that certain risk factors make this co-occurrence more likely.
METHODS
Search Strategy
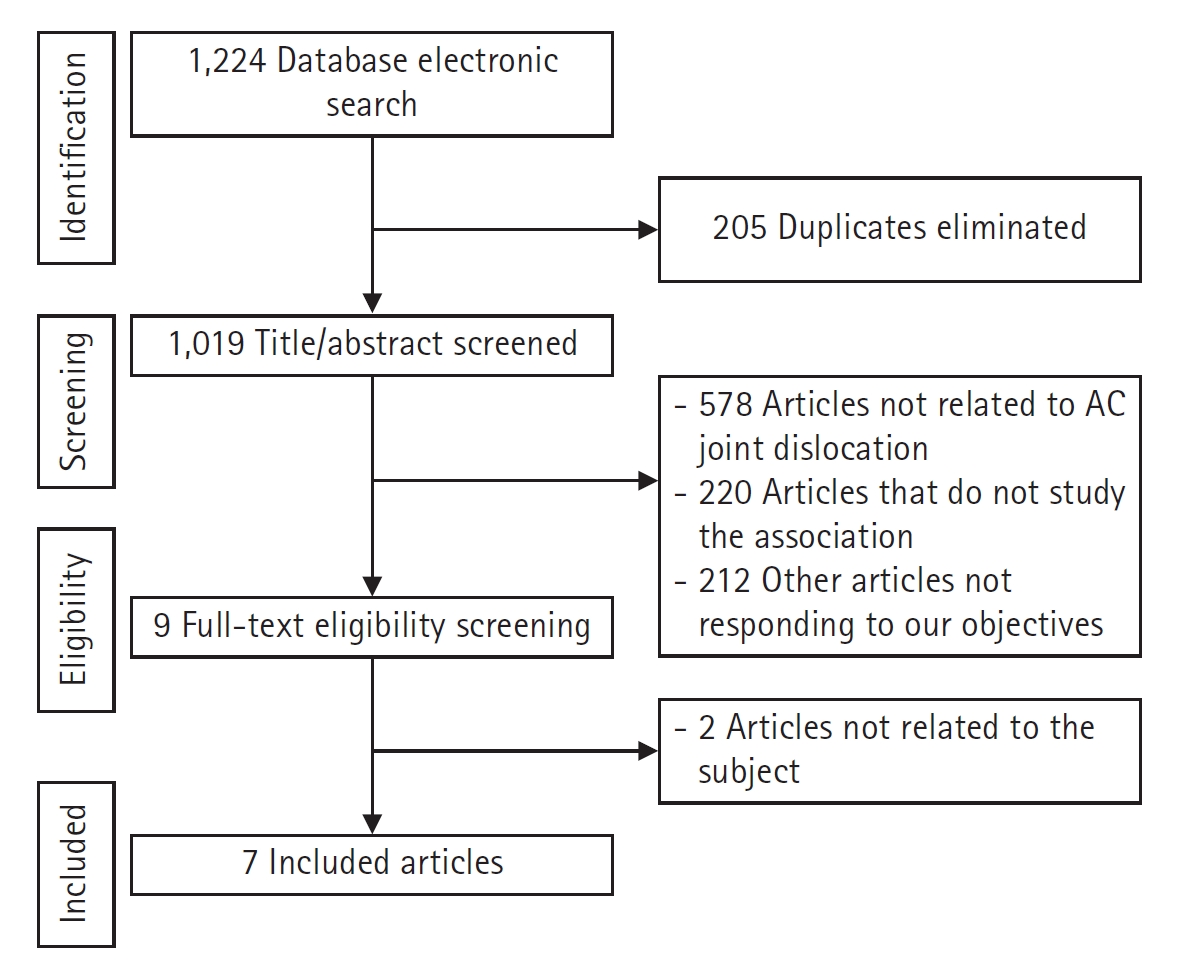
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards were followed in this investigation to study the association between AC joint dislocation and labral tears. Searches in PubMed, Cochrane, and Google Scholar (page 1ŌĆō20) were conducted between 1976 and May 19, 2023, to identify qualified papers. A search query was formulated utilizing Boolean operators by combining MeSH (Medical Subject Headings) terms and keywords ŌĆ£AcromioclavicularŌĆØ OR ŌĆ£ACŌĆØ AND ŌĆ£labrumŌĆØ OR ŌĆ£labralŌĆØ OR ŌĆ£gleno*.ŌĆØ The literature search was complemented by examining reference lists from selected papers. Both title and abstract screening, as well as full-text screening, were independently conducted by two researchers (MD and JEN). Any discrepancies between the two researchers were resolved by consultation with a third investigator (JM). The PRISMA flowchart provides a summarized overview of the article selection process (Fig. 1).
The inclusion criteria were as follows: (1) randomized controlled trials, prospective clinical trials, retrospective studies, and case series and (2) studies where patients had both AC joint dislocation and labral tears. Studies with the following characteristics were excluded from this study: (1) case reports, narrative or systematic reviews, theoretical research, conference reports, expert comments, and economic analyses and (2) studies assessing AC joint degeneration rather than dislocation.
Data Extraction
Data extraction from the selected studies was also performed independently by two reviewers (MD and JEN) and comprised two components. The initial part encompassed essential details such as author names, publication year, journal information, study design, sample size, and potential biases in each study. The second component focused on the prevalence of the investigated relationship and its potential determinants, particularly age and AC joint dislocation grades. Any discrepancies between the investigators were resolved through discussion.
RESULTS
Prevalence of the Association
Pauly et al. [11] conducted a level IV, case series, prognostic study in which they evaluated the prevalence of glenohumeral injuries concomitant with acute grade III or V AC joint dislocations. Of 125 patients, 38 (30.4%) had glenohumeral pathology in addition to their AC joint dislocation [11]. Nine of the 38 patients suffered acute injuries (7.2%) along with the AC joint dislocation, including a superior labrum anterior to posterior (SLAP) type I lesion in one patient and a posterior labral tear in another. Eighteen patients developed degenerative glenohumeral pathologies, among whom five had an SLAP I tear and one had a SLAP III tear [11]. The remaining 11 patients were placed in the intermediate concomitant glenohumeral injuries group due to the unclear relationship between their injury and AC joint dislocation; none of the injuries in this group was a labral tear [11].
Another level IV case series study by Shah et al. [6] enrolled 62 patients with acute AC joint separation. A concomitant IAP was diagnosed in 48 patients (77.4%) using magnetic resonance arthrography (MRA); these pathologies included SLAP lesions (72.6%) and tears of the anterior (24.2%) and posterior labrum (4.8%). The SLAP tears varied in type and prevalence, with type 1 constituting 31.1% of lesions, type 2 66.7%, and type 3 2.2%. Furthermore, four of the 14 patients with SLAP 1 tears presented with a second labral tear (2 anterior, 2 posterior) [6]. Similarly, the incidence of concomitant IAP in patients with Rockwood grades III through V AC joint dislocations was identified in a case series conducted by Tischer et al. [2]. The study comprised 77 patients, of whom 14 (18.2%) had intra-articular injuries identified alongside the AC joint dislocation. Eleven of these 14 patients had SLAP tears, with three being type 1, two type 2, three type 3, and three type 4 [2].
In a non-randomized prospective case series conducted by Pauly et al. [10], the prevalence of concomitant IAPs was investigated in patients treated arthroscopically for Rockwood grades III, IV, and V. The study included 40 patients, of whom six sustained traumatic intra-articular lesions (15%). Among them, two patients had a type II SLAP lesion, and one had a type IV SLAP lesion. Moreover, hemarthrosis was absent in SLAP tears, which is not the case with rotator cuff tears [10]. Ruiz Ib├Īn et al. [12] conducted a retrospective observational multicenter study to assess the prevalence of IAPs concomitant with acute AC joint separations of Rockwood grades III, IV, V, and VI. Among the 201 patients enrolled in their study, 28 (13.9%) had accompanying intra-articular lesions with their AC joint injury (ACJI). Of these lesions, 16 were of labral origin, six anteroinferior labral lesions, three anterior labral lesions, one posteroinferior labral lesion, four type II SLAP tears, and two type I SLAP tears [12].
Additionally, in a retrospective study led by Jensen et al. [13], there was increased risk of IAPs concomitant with ACJIs grade III or V. A total of 376 patients was included in the study sample, of whom 229 were defined as having an acute ACJI (0ŌĆō21 days after trauma) and 147 patients as having chronic ACJI (>21 days after trauma) [13]. Among these 376 patients, 317 (84%) had concomitant IAPs and 201 (53%) had at least one additional glenohumeral pathology [13]. Labral lesions were seen in 73 patients, SLAP I lesions in 60, and SLAP II lesions or higher in 20.
Furthermore, in a retrospective study conducted by Markel et al. [1], the incidences of concomitant IAP in patients with Rockwood grades III, IV, and V AC joint dislocations were identified. The study included a total of 163 patients in whom 28 (17.2%) had an associated SLAP tear [1]. The data highlight a significant but variable occurrence of IAPs in AC joint dislocations. The pooled prevalence of intra-articular labral injuries associated with acute AC joint dislocation was 27% (including 282 labral injuries in 1,044 patients with acute AC joint dislocations). This variation is especially pronounced when considering the specific grade of ACJI. The prevalence of intra-articular labral injuries associated with AC joint dislocation ranged from 13.9% to 84.0% depending on the study and the grade of AC joint dislocation. Notably, SLAP lesions were frequently identified as the predominant type of labral tear. The prevalence of SLAP tears in patients with AC joint dislocations also varied across these studies depending on the grade of ACJI. The prevalence ranged from 7.2% to 77.4%, with higher grades of AC joint dislocations often associated with a higher prevalence of SLAP tears. Consequently, there is a clear need for a comprehensive understanding of IAP prevalence that accounts for the ACJI grade, which can aid in refining the diagnostic and treatment strategies for ACJIs.
Possible Risk Factors
Tischer et al. [2] found that no SLAP tears were present in cases of Rockwood grade III AC joint separation, and only three presented with Rockwood IV separations. The remaining eight patients with SLAP tears had a grade V AC joint dislocation. However, Pauly et al. [11] found no differences in the frequency or type of concomitant IAP associated with the AC joint separation across the Rockwood grades (III, IV and V). Moreover, Markel et al. [1] showed in a subgroup analysis that there is no difference concerning the etiology, type, or frequency of concomitant injuries during AC-separation by sex or Rockwood grade.
The incidence of IAPs in AC joint dislocations varied across Rockwood grades, with SLAP tears primarily associated with grade V dislocations. Every case of grade V dislocation (100%) presented with SLAP tears. In contrast, there were no significant differences in the frequency or type of IAP among Rockwood grades III, IV, and V. Furthermore, patients suffering from a SLAP tear alongside their AC joint separation were, on average, older than the average age of the studied group, although the trend was not statistically significant (42.1 vs. 35.5 years, P=0.58) [2]. However, neither Shah et al. [6] nor Ruiz Ib├Īn et al. [12] demonstrated a significant association between age and the prevalence of concomitant labral tears (P=0.36 from Shah et al. [6]). The analysis of risk factors of IAPs in AC joint dislocations provides valuable insights into patient demographics and injury patterns. However, studies did not find significant differences in the prevalence of labral tears by age. This finding highlights the need for further research to establish a clearer understanding of these risk factors and their clinical implications [2,6,12].
DISCUSSION
The prevalence of concomitant labral injuries and AC joint dislocation was approximately 27%. This prevalent association may be explained by the shared mechanism of injury in these two entities. Direct or indirect trauma is the most common cause of AC-joint separations, which often result from a fall, accident, or direct blow to the upper extremity with scapular depression [6]. Alternatively, an indirect injury can cause AC-joint separation because impact on the adducted hand or elbow drives the humeral head into the acromion [14]. These same mechanisms of injury can also damage active or passive stabilizers, such as muscle attachments, ligaments, labrum, and bony or cartilaginous structures. Similar mechanisms may lead to compression or traction injuries (in the case of traumatic SLAP lesions), which are frequently caused by a fall to the abducted or flexed arm [15-17]. These phenomena can explain the association between ACJIs and labral lesions. Furthermore, Clavert et al. [18] demonstrated in a biomechanical study that SLAP type II lesions occurred in every simulated fall onto outstretched arms. In that study, a customized shoulder testing device that can imitate muscular stresses was attached to a servohydraulic testing system and used on 10 cadaveric shoulders to simulate a forward or backward fall [18]. Five SLAP lesions were discovered in the five shoulders used to simulate a forward fall. In contrast, only two SLAP lesions were identified in the five shoulders that were used to simulate backward falls. Shearing forces appeared to play a significant role in the development of this injury [18].
AC-joint reconstruction is performed solely through an all-arthroscopic trans-articular approach, and diagnostic shoulder arthroscopy is also conducted in these cases. However, for surgeons who use an open approach for AC-joint repair, preoperative MRI scans may be useful to determine which patients should undergo arthroscopy before the open procedure. For instance, Shah et al. [6] employed MRA, which has a reported sensitivity ranging from 89% to 100%, specificity ranging from 69% to 91%, and accuracy ranging from 74% to 92% for the detection of labral/SLAP lesions. Therefore, MRA may be an important diagnostic modality that clinicians should consider when it is clinically available [19-21]. Although an acute physical examination may be unreliable, routine use of MRA in the setting of acute AC joint separation may not be fiscally feasible and should be reserved for cases in which non-operative management has failed.
As for possible risk factors, the findings are still contradictory and inconclusive. Shah et al. [6] found no significant age difference between patients with and without concomitant labral pathologies. This was also demonstrated by Ruiz Ib├Īn et al. [12] and Tischer et al. [2], who showed that the prevalence of associated lesions was not correlated with the subjects' sporting activity level, work site functional requirements, or age. Furthermore, Markel et al. [1] and Pauly et al. [11] did not find any difference in the frequency of associated labral lesions between the different Rockwood types. However, according to Tischer et al. [2], there is a greater incidence of SLAP lesions in cases of Rockwood type V than there is in milder forms of AC joint instability.
Clinicians face several challenges when analyzing the association between AC joint dislocation and intraarticular pathologies. First, it is difficult to differentiate between pre-existing, asymptomatic labral lesions and those that were caused by the same trauma that caused the ACJI [11,22]. In fact, several studies have revealed that previous injuries or overuse may result in asymptomatic findings that can lead to unnecessary treatments [23-25]. Nevertheless, Pauly et al. [11] found that only a small proportion of IAPs (14.4%) in high-grade AC separation cases were unrelated to recent trauma based on the tissue appearance during arthroscopic surgery. This problem is even more prevalent in low grade AC joint dislocations. According to Mouhsine et al. [26], approximately 27% of grade 1 and 2 AC separation cases treated nonoperatively required additional surgery. Another study by Petri et al. [27] showed that more than 65% of patients who failed nonoperative management of grade 3 AC separation had intra-articular pathologies (IAPs) identified during eventual operative management. Since nonsurgical treatment is the primary method of managing low-grade AC joint separation, there is limited literature on its associated pathologies [1]. Second conducting a thorough examination of an acute AC separation can be difficult because it requires painful restriction of shoulder motion and strength. In addition, the clinical tests for SLAP tears are similar to those used for AC separation [6]. Furthermore, it is currently uncertain whether repair is necessary for these injuries, such as partial tears of labral structures, which may heal without surgery. Additionally, there is a lack of data on revisions after failed AC-joint repair due to overlooked intra-articular pathologies that may be due to the injury but are not problematic enough to require revision surgery [10]. However, ongoing shoulder pain after successful AC-joint repair may be caused by other injuries. It is the surgeonŌĆÖs responsibility to identify and treat these accompanying injuries [10].
This study has several limitations. For instance, there was a small number of included studies despite the extensive search method used across three databases. Furthermore, the inclusion and exclusion criteria for patients were different. The data used for the analysis were pooled, and the individual patient data were unavailable, which could have limited comprehensive analyses. Regardless, this was the first systematic review studying the prevalence of the association between acute AC joint dislocation and labral tears.
CONCLUSIONS
Our findings shed light on the intricate relationship between labral lesions and AC joint dislocations, which have a prevalence of approximately 27%. Notably, SLAP lesions emerged as the predominant type of labral tear and exhibited a grade-dependent pattern. Higher-grade AC joint dislocations are often associated with a higher prevalence of these tears. However, it is unknown whether these labral injuries were caused by the AC injury itself, or if they were present prior to the dislocation. Therefore, further high-quality research is warranted to clarify this prevalent association.