INTRODUCTION
A seizure disorder (SD) is an adverse clinical event attributed to improper electrical discharge in the brain [1]. Several causes for seizures have been described; of these, epilepsy, substance abuse, hypoglycemia in diabetes, and adverse drug reactions are prime causes of recurrent shoulder dislocations (0.6%) [2,3]. The spectrum of shoulder injuries in SD patients ranges from index dislocations to recurrent instability [1]. The mechanism of SD-associated anterior and posterior shoulder dislocations has been well described [1]. SDs are the most common cause of recurrent posterior shoulder dislocation [1], and recurrent anterior shoulder dislocations (RASDs) are the most common type of shoulder dislocation in SDs [1]. Recent studies have reported the incidence of RASD to range from 65% to 86% [4-7]. The problems unique to RASD in SDs are 1, a large anterior bony Bankart lesion; 2, an engaging Hill-Sach's lesion; 3, significant attritional bone loss; 4, osteoporosis of the glenoid and humeral bones under the effect of anti-epileptic medications; 5, a history of irregular treatment; 6, associated psychiatric disorders; and 7, a history of substance abuse [7]. The treatment options for recurrent instability due to SDs include the Putti-Platt procedure, Bankart's repair with/without remplissage, capsular shift, bone block procedure, coracoid transfer, glenoid neck/humeral osteotomy, arthrodesis, and arthroplasty [7]. Recent investigations have narrated management options for recurrent shoulder instability; however, the studies did not follow methods of systematic search and critical appraisal [4,5,7]. The primary objective of this review was to analyze the safety and efficacy of operative interventions for recurrent anterior dislocation in SD.
METHODS
The procedures followed in this review adhered to the ethical standards of the responsible committee on human experimentation (institutional and national). This review was registered with the PROSPERO International Prospective Register of Systematic Reviews and followed the Preferred Reporting Items for the Systematic Review and Meta-analysis (PRISMA) (CRD42023457738) guidelines [8]. The authors obtained informed consent from the authorities at the institute/organization where the work was carried out.
Eligibility Criteria
We included reports published in English that studied operative interventions for RASD in SD patients. Studies were included in this review irrespective of the cause of SD or the type of operation (soft tissue/bony/arthrodesis/arthroplasty). Case reports, studies on nonoperative treatment, studies with neglected and missed dislocations, and reports of fractureŌĆōdislocations resulting from SD were excluded from this review. Studies describing heterogeneous treatment methods and mixed reports reporting the treatment of RASD with SD as one of the causes also were excluded.
Information Sources
Major electronic databases were searched up to August 2023 to identify studies published in the English language on the treatment of RASD in SD.
Search Strategy
We searched the Cochrane Library, Embase, PubMed, the Directory of Open Access Journals, ProQuest, and Scopus on August 19, 2023. Supplementary Material 1 describes this review's search strategy for electronic databases. We hand-searched the references of initially included studies. We excluded reports from trial registries, conference proceedings, books, and dissertations.
Selection Process
Rayyan intelligent systematic review website (Rayyan Systems) was used to manage the search results. Review authors (DC and AR) independently screened all titles and abstracts for potentially eligible studies, obtaining full-text reports when was it appropriate. The same two review authors independently performed study selection. We resolved disagreements about the inclusion or exclusion of individual studies and data extraction by discussion between the two authors or with a third author (SKN) for the final study selection to ensure a consensus. The data collection included study design, population, interventions, outcome measures, and results. We did not mask the source or authorship of the trial reports. The reviewers used a pre-defined Microsoft Excel data-collection sheet (Microsoft Corp.) to extract relevant data.
Data Items
The following characteristics from the included reports were recorded. 1: Complications, including failure defined as recurrence of dislocation in a treated case, screw fracture/bending, recurrence of SD in follow-up, and non-union/fracture of the coracoid process; 2: functional outcome measures of the shoulder joint, including the Oxford shoulder instability score, Constant and Murley scores, and Rowe score; 3: demographic outcomes of age, sex, bilaterality of operation, and types of implants as well as number of dislocations before the operation and duration of epilepsy; and 4: radiographic outcomes of bony lesions on the humeral head (Hill-Sach's lesion) and glenoid erosion (bony Bankart lesion).
Assessment of the Risk of Bias in Included Studies
We did not assess studies for risk of bias due to the rarity of anterior shoulder instability in seizures and diverse treatment methods and study designs. However, consecutive and complete inclusion of participants was unconfirmed in the three included case-control studies, placing them at risk of bias [6,9,10]. One of the case-control studies also did not report the presenting sites/clinics demographic information [9]. Finally, one case-control study [6] included retrospective data from matched cohorts of cases and controls, while the other two did not [9,10].
Effect Measures
Continuous data were summarized as mean with standard deviation or median with interquartile range. Each variable was compared between groups, excluding cases with missing data. A forest plot was constructed using the proportions of events in the case and control groups, respectively. The effect estimate was the risk rate with 95% confidence interval. A fixed-effects model pooled the risk of failure/recurrence of dislocation from case-control studies on the Latarjet operation for RASD. The heterogeneity and inconsistency across included studies were assessed using the chi-square test and I2 test. Statistical inferences were based on a two-sided significance level of P<0.05. All analyses were performed using Stata v14.0 (StataCorp.). A review author (SKN) performed the statistical assessments.
RESULTS
Qualitative Analysis
Study selection
We searched 500 records until August 2023 for studies on operative interventions for treating RASD in SD patients. The Cochrane Library (0), Medline (61), Embase (96), PubMed (64), ProQuest (43), Scopus (214), and the Directory of Open Access Journals (22). We isolated 19 studies meeting the inclusion criteria from electronic databases [2,3,5,6,9-23]. The full texts of these 19 studies were analyzed and revealed three additional studies to include [15,17,22]. Eight studies were excluded from the qualitative and quantitative analyses [2,5,9,13,16,17,20,22]. Fig. 1 shows the reasons for study exclusion. We analyzed 11 qualitative analyses [3,6,9,10,12,13,15,16,19,20,22] and three meta-analyses [6,9,10]. The PRISMA flow diagram for this review also is presented in Fig. 1.
Based on the type of treatment reported in the included reports, we divided the selected studies into four groups: group 1: soft tissue procedure (BankartŌĆÖs operation with remplissage [12], group 2: Latarjet and Bristow operations [3,6,9,10,16], group 3: bone block operations (autograft and allograft) [13,15], and group 4: arthrodesis [18,19] and arthroplasty [20,22].
Group 1: qualitative analysis of soft-tissue procedures for the treatment of RASD
One retrospective cohort study investigated the effects of Bankart operation with remplissage in SD-associated RASD [12]. The patients in that study had medically controlled epilepsy, were free from SD for at least 1 year [12], and underwent surgery at a mean of 25.4┬▒3.8 months (18ŌĆō32 months) after their last SD episode. The minimum follow-up of the included cases was 2 years, and all included patients experienced an average glenoid bone loss of 12.1%┬▒8.9% (0%ŌĆō18%) on computed tomography (CT) imaging. The outcomes of the study are summarized in Table 1.
Group 2: qualitative analysis of the Latarjet operation for RASD in SDs
We pooled 106 cases/118 shoulders from five studies that investigated the effects of Latarjet operation for RASD in SD patients [3,6,9,10,16]. The pooled outcomes are summarized in Table 1. This group included two case series [3,16] and three retrospective case-control studies [6,9,10]. SDs from epilepsy [6,9,10,16] and substance abuse (tramadol) [3] were studied in four and one reports, respectively.
The mean duration of tramadol addiction was 17┬▒9 months (5ŌĆō40 months). The cases/shoulders (57/62) in the described study were recruited after a rehabilitation program that included detoxification confirmed by serial dipstick urine testing [3]. The bipolar bone loss at the humeral head and glenoid was estimated on CT as 26%┬▒6% (15%ŌĆō40%) and 24%┬▒6% (15%ŌĆō35%), respectively [3]. There were eight failed operations before inclusion of patients in the study [3]. Tramadol-induced SD recurred in five cases. The Rowe scores improved significantly in all participants after the operation. There were three failures after the Latarjet operation.
Another case series (12 cases/14 shoulders) recruited patients without medical control of SD [16], with a mean of 5 years (0.8ŌĆō9.3 years) between the onset of epilepsy and first dislocation. The Latarjet operation was performed at a mean of 6.5 years (0.5ŌĆō35 years) after the first dislocation. Three Bankart operations per shoulder failed in two cases before the Latarjet operation. The bipolar bone loss was quantified on x-rays [16]. The study reported six failures (43%) at a mean of 2.2 years (1.2ŌĆō4 years) after the Latarjet operation [16], all of which were managed by bone block operation. SDs recurred in 25 cases/26 shoulders after the Latarjet operation in group 2, resulting in 16 failures. Twelve hardware complications (screw breakage/bending) were recorded in group 2 due to the recurrence of SD after the Latarjet operation [3,6,9,10,16].
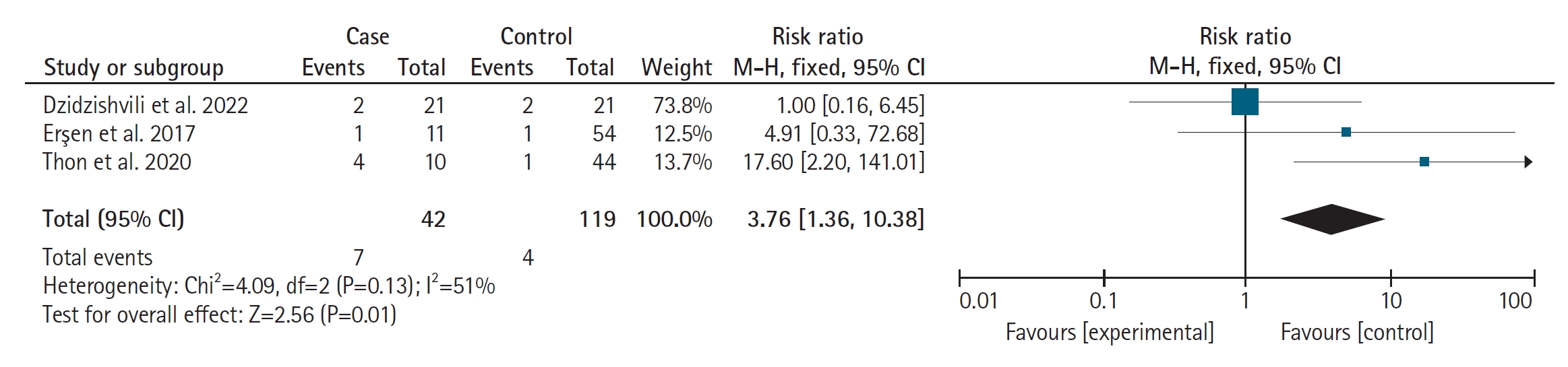
A comparative summary of pooled outcomes between cases and controls is presented in Table 2. All the case-control studies included participants with a minimum of 2 years of follow-up [6,9,10]; however, they were diverse in several other outcomes. While one study [9] reported a mean onset age of epilepsy of 15 years, the others did not report an onset age [6,10]. One case-control study described the duration between the first dislocation to Latarjet operation as a mean of 21.3┬▒4.5 and 21.4┬▒3.5 months for cases and controls, respectively [6]. Two studies recorded the occurrence of four and six failed Bankart operations before the Latarjet procedure in cases and controls, respectively [6,10]. All the case-control studies estimated bone loss using CT imaging. While one study commented on Hill-Sachs lesion presence in all cases [16], the other measured a mean depth of 24.7├Ś4.4 mm and 23.7├Ś5.2 mm in cases and controls, respectively [6]. One study reported 20 and 21 off-track Hill-Sachs lesions in cases and controls, respectively [6]. The studies were diverse in reporting the details of glenoid erosion in cases and controls: one study simply documented the presence of glenoid erosions in nine cases and 41 controls [9], while another measured glenoid erosion to be 3.1┬▒3.4 mm and 2.1┬▒ 2.4 mm in cases and controls, respectively [6]. Two studies [6,9] commented on the medical treatment of epilepsy, while one did not [10]. Two failures after the Latarjet operation were managed with the Eden-Hybinette procedure [6,9], while one failure in a control was managed by distal tibia allograft [10]. Five cases from two studies had hardware complications of screw breakage or bending due to recurrence of SD [9,10]. Overall, 12 cases (15 shoulders) experienced SD recurrence, resulting in seven failures after the Latarjet operation [6,9,10]. The relative risk of recurrence of dislocation/failure between cases and controls is presented in Fig. 2.
Group 3: qualitative analysis of the bone block procedure for treating RASD
This group included two retrospective case series that treated recurrent dislocations in epileptic patients with bone block operation [13,15]. The pooled outcomes of the included studies are presented in Table 1. One study with eight shoulders/cases investigated the outcomes of the Eden-Hybinette procedure using an autologous iliac crest in revision cases with medical control of epilepsy [15]. There were four and two failed Latarjet/Bristow cases and arthroscopic Bankart's procedures among the included cases, respectivcely [15]. Two cases failed to resolve with both procedures [15]. All cases underwent CT estimation of glenoid bone loss, and all demonstrated greater than 25% loss [15]. An off-track Hill-Sachs lesion was reported in all humeral heads [15]. There was no SD or recurrence after bone block operation at a mean follow-up of 2.65┬▒2.94 years (0.75ŌĆō4 years) [15].
Another study examined the outcomes of bone block operation in 13 epileptic patients/15 shoulders [13]. The study investigators used larger bone grafts compared to Eden-Hybinette procedure to create a smooth anterior extension of the glenoid [12]. The study included a mean of 46 (4ŌĆō120) dislocations per shoulder before the bone block operation [13]. In all cases, the glenoid bone loss estimated on x-rays was one-third of normal [13]. Three, three, and six failed Bankart repairs, Bristow procedures, and Putti-Platt operations, respectively, occurred before inclusion in the study [13]. All patients had uncontrolled epilepsy, and the operation was delayed until control improved. There was a recurrence of SD in eight cases [11,13]; however, no failures were reported, and the functional outcome scores of shoulders improved after the operation. The salient features and outcomes of studies in group 3 are summarized in Table 1.
Group 4: qualitative analysis of arthroplasty for treating instability arthropathy due to RASD in SD patients
We pooled 11 shoulders/cases of instability arthropathy due to RASD from SD in group 4 [20,22]. The two included studies were retrospective case series from one center that recruited patients with grand mal SD with recurrent shoulder instability. Two cases in which arthroplasty was performed for posterior instability were excluded from this review [20]. The mean duration of epilepsy was 16.5┬▒21.92 years (4ŌĆō51 years). The included studies reported a mean of two failed operations (0ŌĆō5) per shoulder before arthroplasty. Both the studies evaluated humeral and glenoid bone loss by CT and diagnostic arthroscopy to be compatible with that of arthroplasty before the operation. While one study [22] reported two Putti-Platt, two Bankart, two coracoid transfer, three allograft humeral head reconstruction, and one humeral headŌĆōresurfacing operations before reverse shoulder prosthesis operation, another did not specify the types of operations that failed [20]. Five, four, and two reverse shoulders fixed with a fulcrum arthroplasty prosthesis, humeral head resurfacing, and total shoulder prosthesis were included, respectively [20,22]. Six cases experienced SD recurrence after arthroplasty despite medical management of epilepsy [20], but there were no failures in either study. The ranges of forward flexion and external rotation improved in all cases. One study reported two complications unrelated to dislocation recurrence [20]. The outcomes of studies included in this group are summarized in Table 1.
Qualitative Analysis of Arthrodesis in Instability Arthropathy Following RASD
One retrospective case series reported the effects of glenohumeral arthrodesis in six shoulders/cases with RASD [19]. The included cases had bone loss enough to preclude arthroplasty/bony/soft-tissue reconstructive procedures, and all cases had medial bone loss extending up to the coracoid process. The included patients were receiving medical management for epilepsy. All cases achieved fusion at a mean of 2.8 months (2ŌĆō7). Though SD recurred in five cases after glenohumeral arthrodesis, all participants demonstrated improvement in the Oxford shoulder instability score and subjective shoulder value. One complication in each of the two cases was unrelated to instability. The outcomes of studies included in this group are summarized in Table 1.
Medical control of epilepsy, extent of bone loss from the glenoid, number of failed operations, and instability arthropathy were indications for operation. Medically controlled epilepsy patients with bone loss less than 20% without any history of failed operations are candidates for BankartŌĆÖs operation with or without remplissage. Meanwhile, failed soft-tissue procedures and bone loss greater than 20% in medically controlled epilepsy render a patient a good candidate for the Latarjet operation. When bone loss exceeds one-third of the glenoid diameter with or without multiple failed operations, bone block operation is the procedure of choice. Finally, arthrodesis or arthroplasty is warranted when shoulder arthropathy has set in to preclude any joint-sparing operation.
Meta-Analysis
We estimated a relative risk of failure of 3.76 (1.36ŌĆō10.38) between SD and non-SD patients with RASD after the Latarjet operation (Fig. 2). The seizures recurred after surgery in 33% of the pooled SD-associated RASD cases. The failure rates after Bankart's operation with remplissage and the Latarjet procedure in SD patients were 17% and 13%, respectively, compared to 0% each for the bone block operation, arthroplasty, and arthrodesis. We estimated a moderate heterogeneity of 51% using I2 statistics across the included studies. A graphical representation of the publication bias test is depicted using a funnel plot, which shows the symmetric distribution of the effect estimate, indicating the absence of publication bias (Fig. 3).
DISCUSSION
We determined the risk of failure of the Latarjet operation to be 3.5 times higher in SD patients than in non-SD patients with RASD. Recurrence of SD in the postoperative period remains a significant predictor for failure of Latarjet and Bankart's operations in such patients; however, the same does not hold for patients undergoing bone block operation. Our observations should be interpreted cautiously considering the rarity of RASD in SD and the quality of the included studies. The likely reason for the comparative success of the bone block operation despite seizure recurrence in RASD could be a more robust and thicker allograft/tricortical iliac crest autograft devoid of muscular attachments. A better screw purchase in the tricortical bone compared to the coracoid graft in the Latarjet operation has also been hypothesized [15]. However, the screw diameter was demonstrated not to influence failure [10]. Er┼¤en et al. [9] hypothesized postoperative seizures within six weeks to be a cause for failure of the Latarjet operation; however, Thon et al. [10] reported failures at 3 and 4.5 months and 2 and 2.5 years after latarjet operation failure. The effects of medical treatment on the efficacy of the Latarjet operation have been substantiated by the studies included in this review. While seizures recurred in 67% of cases, resulting in a 43% operation failure rate, in a single study [16] without medical management, the pooled studies revealed a 32% seizure recurrence rate with a 10% failure rate in medically treated RASD cases [6,9,10]. Further, all failures of the Latarjet operation across included studies occurred in seizure recurrence cases.
The rationale behind arthroplasty in instability arthropathy is the poor quality of bone and end-stage cartilage degeneration. Short-term (5-year) follow-up of arthroplasty for end-stage instability arthropathy is an acceptable alternative to arthrodesis if sufficient bone is available for component fixation [11,20,22]. Reports on the role of arthroplasty in instability arthropathy due to seizures have not reported prosthesis dislocation despite the recurrence of seizures [11,20,22]. Austin et al. [11] reported three prosthetic dislocations unrelated to seizures in RASD-associated instability arthropathy in SD. Implant use for arthroplasty was diverse in the studies included in this review. One study used fixed-fulcrum reverse shoulder prostheses [22] in all included participants, while another included cases of total shoulder arthroplasty treated with resurfacing humeral head prostheses [20]. However, in the event of shoulder instability due to SD complicated by ongoing anti-epileptic medications, compromised rotator cuff capsular insufficiency due to multiple operations, or attritional bone loss in the humerus and glenoid to preclude arthroplasty, arthrodesis is an acceptable alternative.
Since RASD in SD is rare, data from retrospective case series and case-control studies are the best evidence available in such patients; however, comparative studies of bone block operation versus the Latarjet procedure in patients not fit to undergo Bankart's operation will further determine the relative efficacy of these procedures.
Limitations of This Review
We identified six studies including 149 shoulders with RASD due to seizures that involved heterogeneous treatment methods and patient populations [2,5,11,17,18,21]. Including these studies could have influenced the outcomes of this review. One study was a multicenter case-control study [2], and another adopted allografting of the humeral head for treatment of RASD in seizures [17]. The clinical and methodological diversity of these studies would have introduced moderate heterogeneity among the included case-control studies for meta-analysis. Although one study recruited matched controls [6], another two included all surgical non-seizureŌĆōassociated recurrent instability patients undergoing the Latarjet procedure as controls [9,10]. Two studies [6,23] required subcritical glenoid bone loss rates of 15% and 13.5% when recruiting patients for the Latarjet operation, while one did not include a limit [9].
CONCLUSIONS
Medical management of SD is important before considering any type of surgical intervention in RASD patients. Although the Bankart and Latarjet operations are established procedures for treating RASD, they are comparatively less efficacious in the presence of SD. Despite the recurrence of seizures after the operation, the bone block procedure appears more efficacious in controlling failures in RASD patients with seizures. Based on the evidence pooled from this review, we recommend bone block operation over the Latarjet procedure. Meanwhile, despite the recurrence of seizures after arthroplasty, the absence of prosthesis dislocations suggests it is an acceptable alternative to arthrodesis in instability arthropathy.